
Diseases of the Cornea — MCQs

On this page
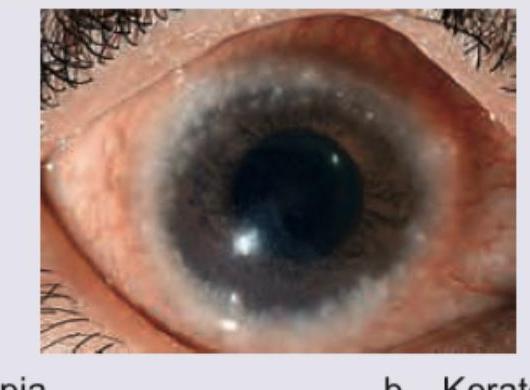
The corneal presentation shown in the image is characteristic of:
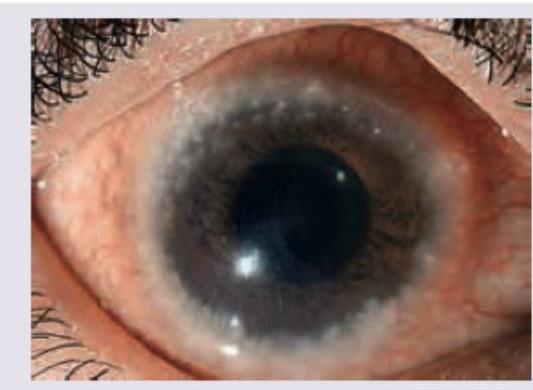
The given image shows presence of:
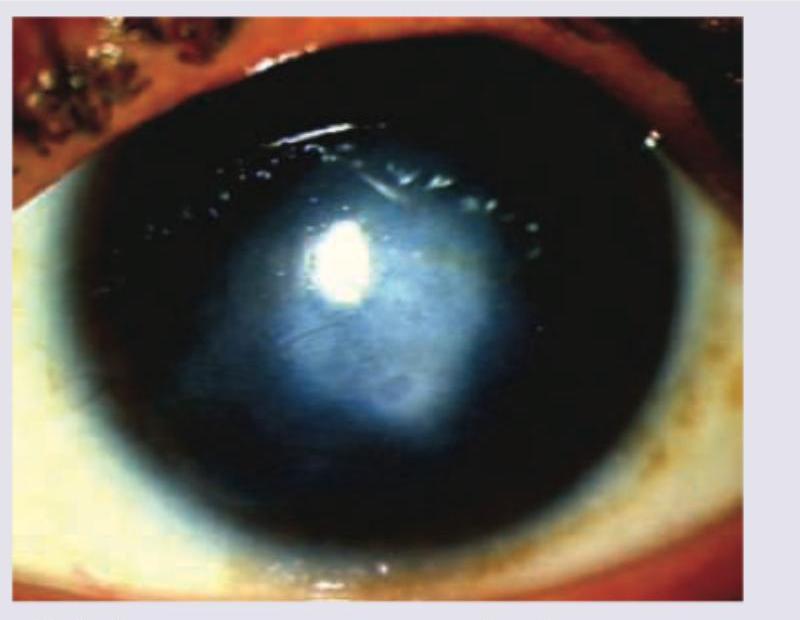
What does the given image show?
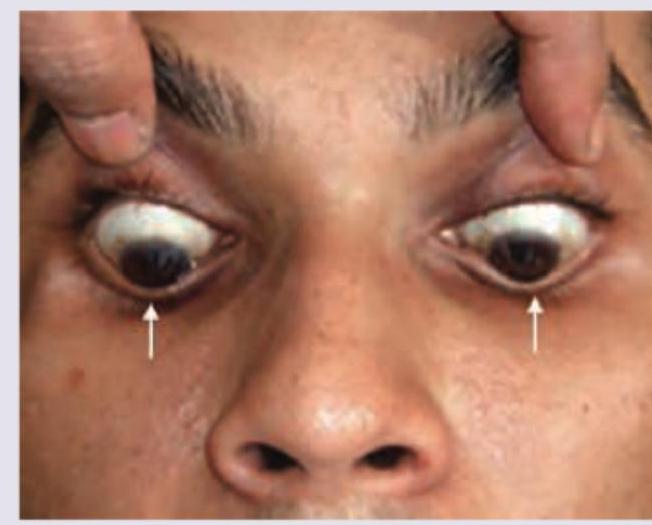
What does the following image show?
All are true regarding the image shown except:

What does the following image show?

A patient presents with a painful red eye. Fluorescein staining reveals the lesion shown in the image. What is the diagnosis?

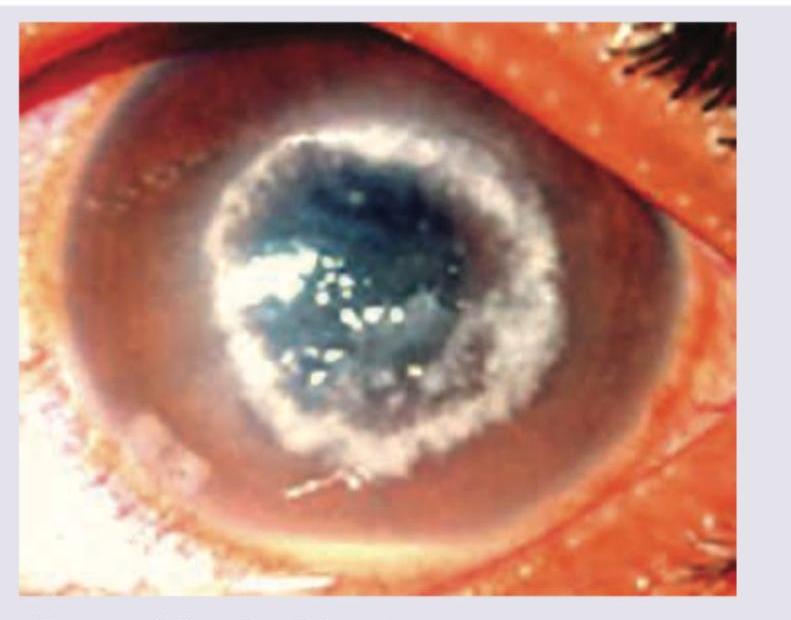
A 15-year-old contact lens user presents with severe eye pain for last 3 days. All are correct about the treatment for the condition shown in the patient except:
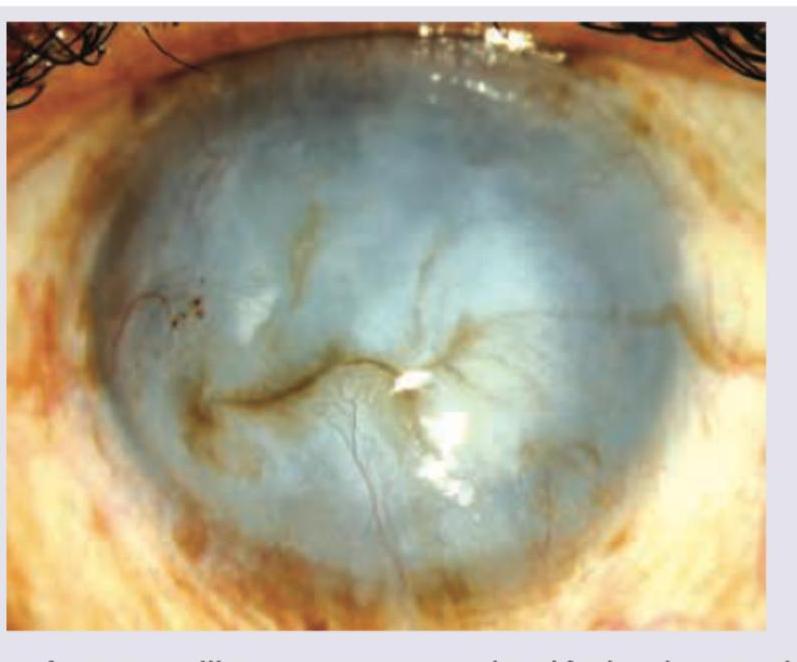
Which complication of the corneal ulcer is shown in the image below?

What does the following image show?
Practice by Chapter
Corneal Anatomy and Physiology
Practice Questions
Bacterial Keratitis
Practice Questions
Viral Keratitis
Practice Questions
Fungal Keratitis
Practice Questions
Protozoan Keratitis
Practice Questions
Corneal Degenerations
Practice Questions
Corneal Dystrophies
Practice Questions
Keratoconus and Ectatic Disorders
Practice Questions
Corneal Transplantation
Practice Questions
Corneal Topography and Imaging
Practice Questions
Dry Eye Disease
Practice Questions
Corneal Trauma
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app