
Diseases of the Cornea — MCQs

On this page
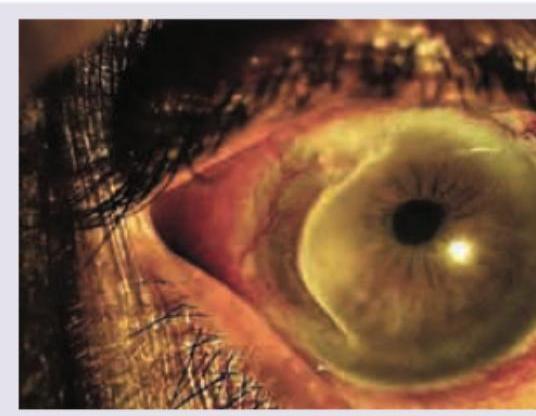
Which is correct about the image shown below?
The corneal image shown below demonstrates a ring infiltrate. What is the most likely diagnosis?
Which is correct about the image shown below?
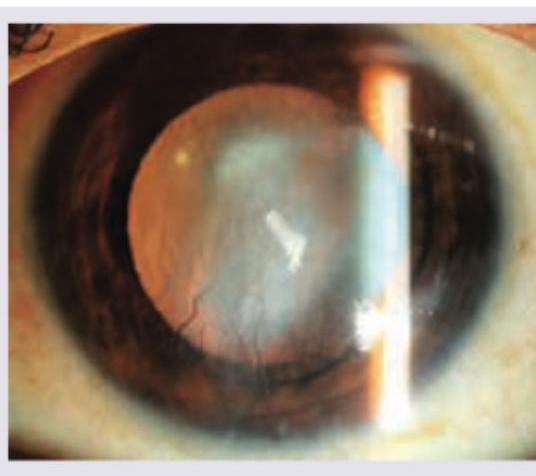
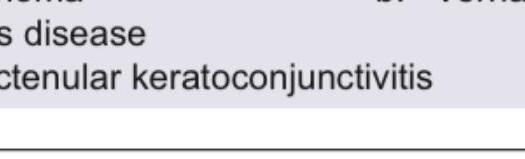
What type of corneal opacity is shown in the image?

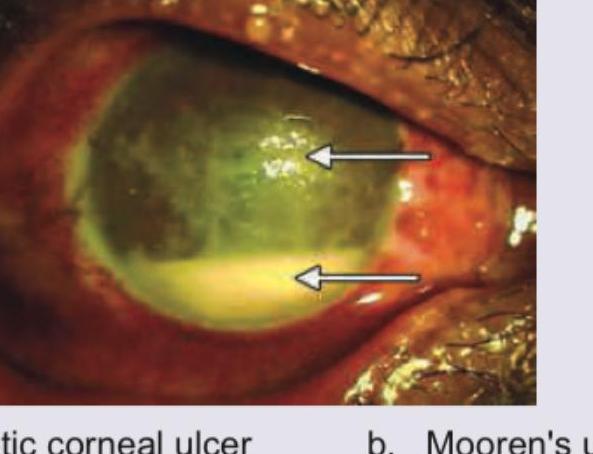
The clinical image shows a corneal pathology. What is the most likely diagnosis?
What is correct about the image shown below?
In a child with juvenile idiopathic arthritis, the eye examination shows presence of:
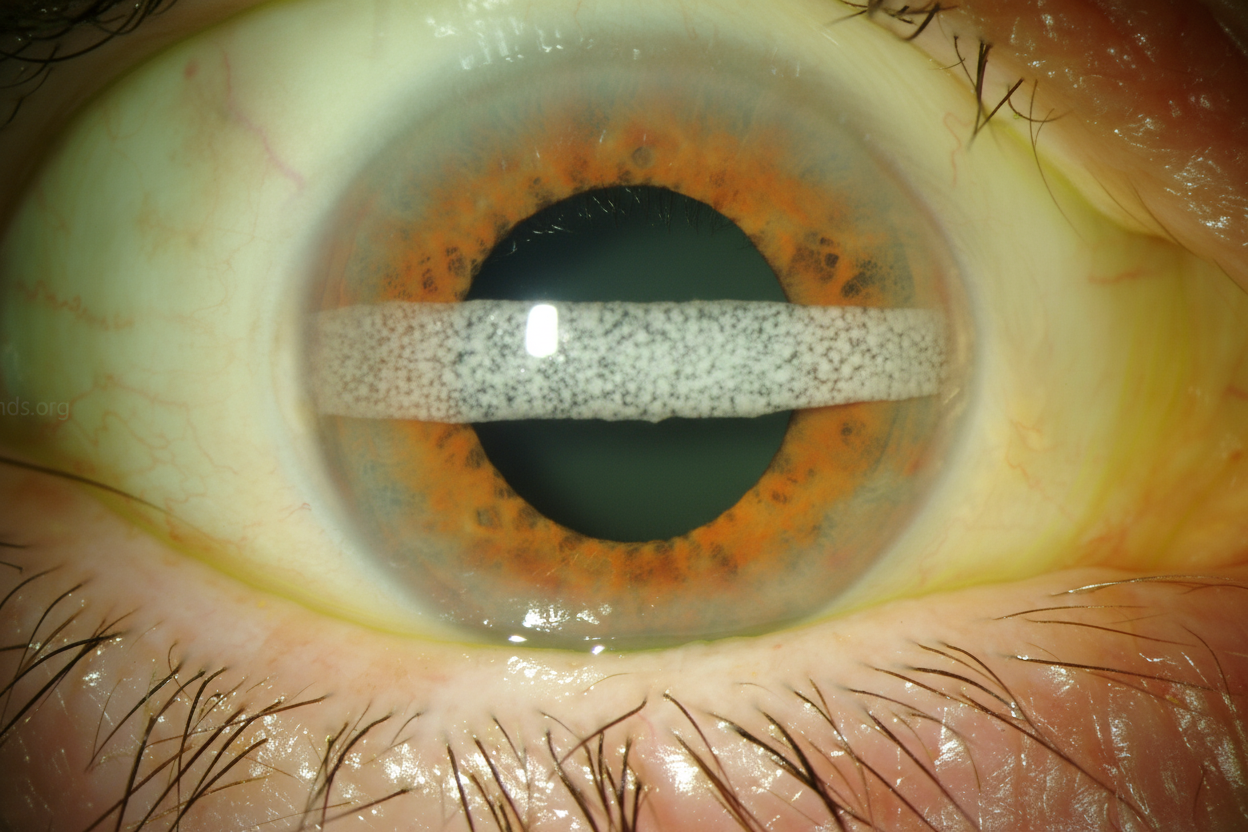
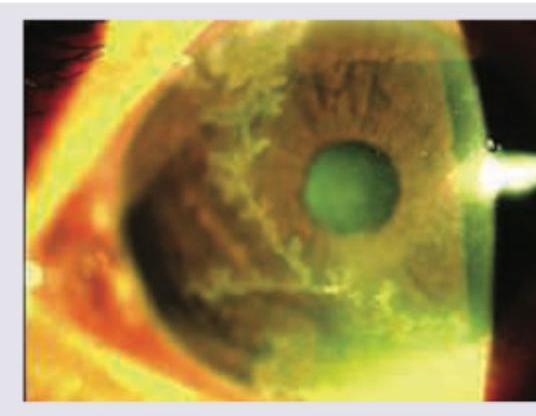
A fluorescein-staining branching epithelial ulcer with terminal bulbs on the cornea as shown below may be seen with:
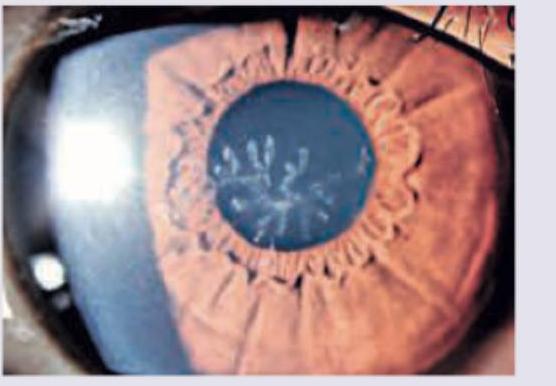
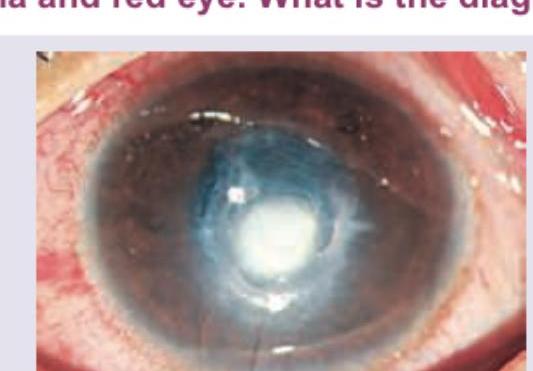
A 30-year-old lady presents with blepharospasm, lid edema and red eye. Based on the clinical photograph shown, what is the diagnosis?
A 30-year-old lady presents with blepharospasm, lid edema and red eye. Examination findings are shown in the image. What is the diagnosis?
Practice by Chapter
Corneal Anatomy and Physiology
Practice Questions
Bacterial Keratitis
Practice Questions
Viral Keratitis
Practice Questions
Fungal Keratitis
Practice Questions
Protozoan Keratitis
Practice Questions
Corneal Degenerations
Practice Questions
Corneal Dystrophies
Practice Questions
Keratoconus and Ectatic Disorders
Practice Questions
Corneal Transplantation
Practice Questions
Corneal Topography and Imaging
Practice Questions
Dry Eye Disease
Practice Questions
Corneal Trauma
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app