
Diseases of the Cornea — MCQs

On this page
Treatment for dendritic ulcer includes all except:
A patient presents to the OPD with a recent onset of photophobia within 24 hours and a sloughing corneal ulcer. There is a greenish ulcer base. Which of the following can be the causative organism?
A patient presents with a painless ulcer in the eye. On examination, a long, branching ulcer with desquamated epithelium is seen on the cornea. What is the most likely diagnosis?
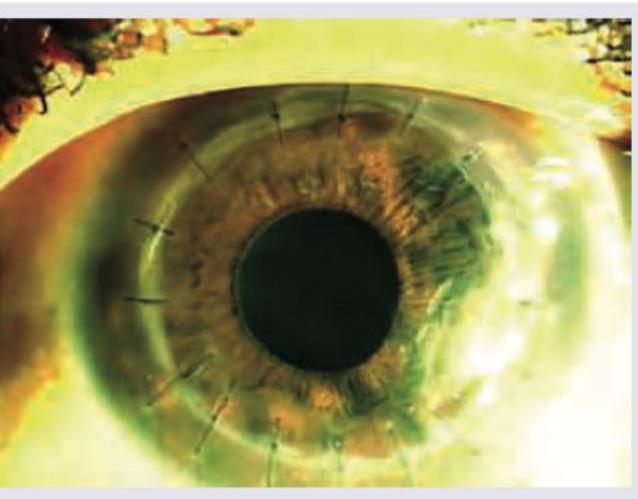
Following a fungal corneal ulcer, a farmer underwent corneal transplant surgery. What is the preservative used for storing the donor corneal graft and the suture material used in the procedure?
Which condition is treated using an Intacs ring, as shown in the image?
A patient presents with guttate lesions in one eye and bullous keratopathy in the other eye. What is the most likely diagnosis?
A child from slums presents with diffuse corneal opacity with softening and melting of the cornea. What is the diagnosis?

The procedure being performed in the image is:

The following appearance of eye is seen in:

Which is correct about the image shown below?
Practice by Chapter
Corneal Anatomy and Physiology
Practice Questions
Bacterial Keratitis
Practice Questions
Viral Keratitis
Practice Questions
Fungal Keratitis
Practice Questions
Protozoan Keratitis
Practice Questions
Corneal Degenerations
Practice Questions
Corneal Dystrophies
Practice Questions
Keratoconus and Ectatic Disorders
Practice Questions
Corneal Transplantation
Practice Questions
Corneal Topography and Imaging
Practice Questions
Dry Eye Disease
Practice Questions
Corneal Trauma
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app