
Diseases of the Cornea — MCQs

On this page
A 25-year-old man presented with a history of pain, redness, and watering of the left eye for the last 1 day. There is also photophobia. What is the most probable diagnosis?
In Herpes zoster keratitis, which of the following clinical presentations is LEAST likely to occur?
Important in Herpes simplex involvement of the eye are all EXCEPT:
A 20-year-old male presents with sudden onset left eye pain and vision loss. Examination reveals a hazy left cornea. Upon looking down, a bulge is noted in the lower eyelid. Retinoscopy demonstrates a scissoring reflex and a positive oil drop sign in both eyes. What is the diagnosis?
Posterior polymorphous dystrophy is characterized by which of the following?
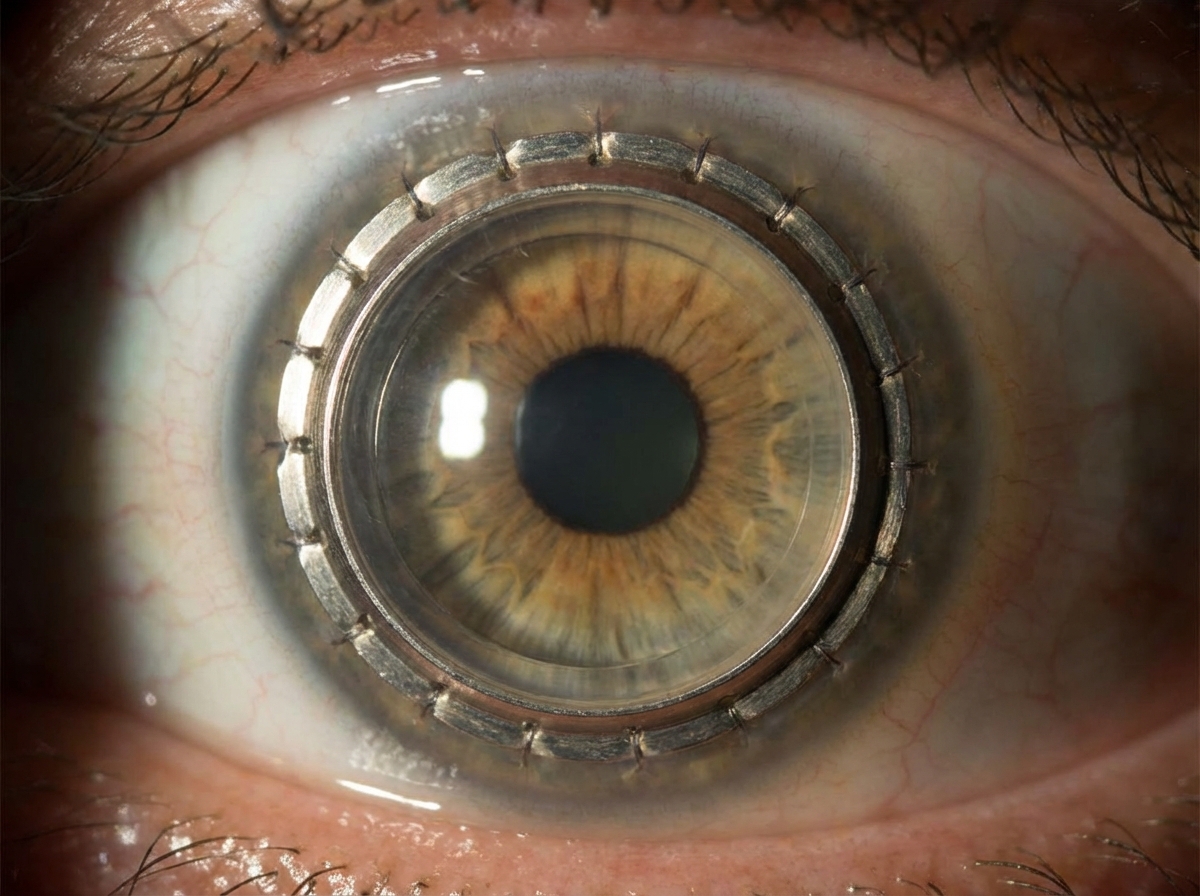
Which of the following is NOT an indication for the Boston type I keratoprosthesis shown in the image?
What is the most common cause of corneal keratitis in soft contact lens users?
Under hypoxic conditions, which of the following is strongly implicated as a cause of corneal edema?
Which of the following medications is NOT typically administered as eye drops for a corneal ulcer?
KISA% is associated with which of the following conditions?
Practice by Chapter
Corneal Anatomy and Physiology
Practice Questions
Bacterial Keratitis
Practice Questions
Viral Keratitis
Practice Questions
Fungal Keratitis
Practice Questions
Protozoan Keratitis
Practice Questions
Corneal Degenerations
Practice Questions
Corneal Dystrophies
Practice Questions
Keratoconus and Ectatic Disorders
Practice Questions
Corneal Transplantation
Practice Questions
Corneal Topography and Imaging
Practice Questions
Dry Eye Disease
Practice Questions
Corneal Trauma
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app