
Diseases of the Conjunctiva — MCQs

On this page
Which of the following conditions can occur in epidemics?
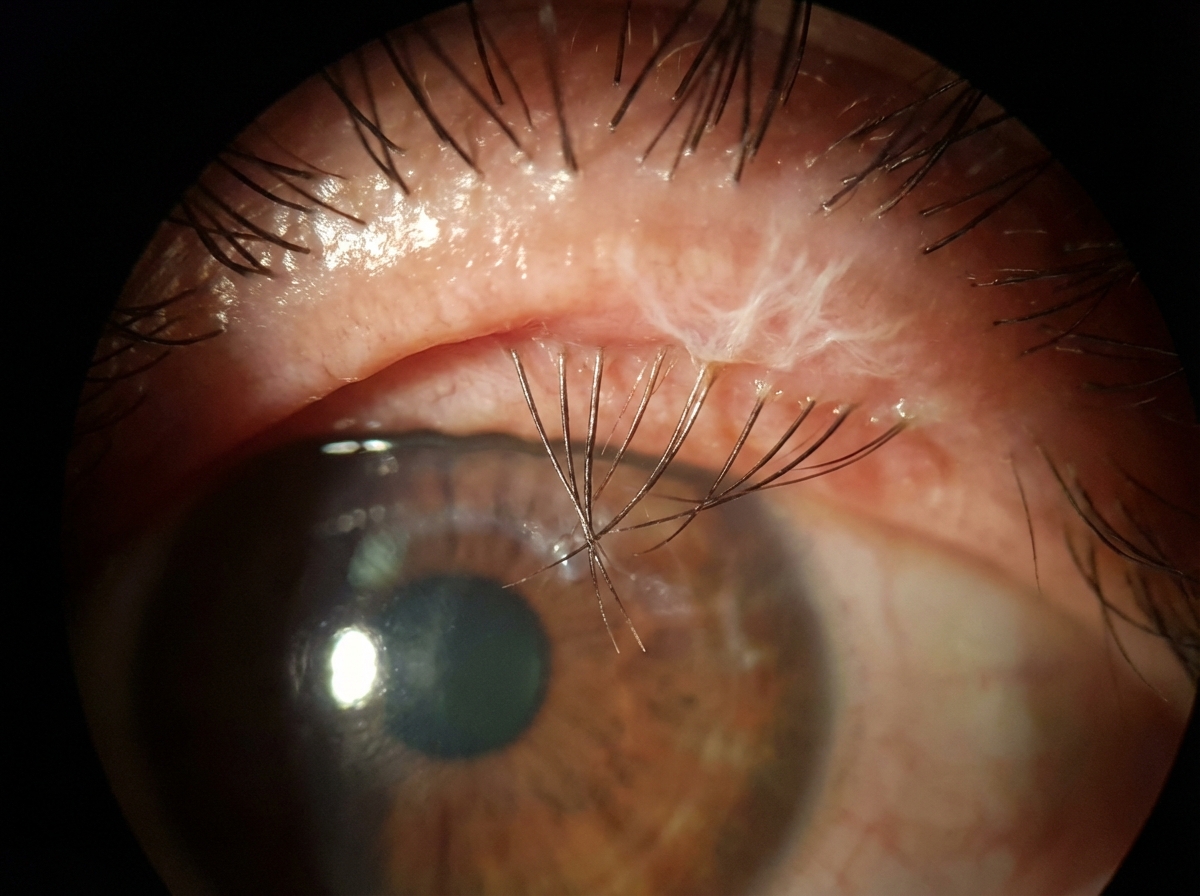
The patient is suffering from which WHO simplified grading sign of trachoma? Note the lashes touching the globe.
What is the primary content of cobblestones in vernal conjunctivitis?
Which of the following is NOT used in the management of ophthalmia neonatorum?
All of the following are known to cause conjunctival xerosis except?
What is the most common cause of ophthalmia neonatorum occurring within the first 48 hours of birth?
Cobblestoning of the conjunctiva is seen in which of the following conditions?
All are seen in stage III trachoma except –
No color change is seen in subconjunctival hemorrhage due to what reason?
Staphylococcal conjunctivitis is associated with all of the following except:
Practice by Chapter
Conjunctivitis: Bacterial
Practice Questions
Conjunctivitis: Viral
Practice Questions
Conjunctivitis: Allergic
Practice Questions
Conjunctivitis: Chronic
Practice Questions
Degenerations of Conjunctiva
Practice Questions
Benign Tumors of Conjunctiva
Practice Questions
Malignant Tumors of Conjunctiva
Practice Questions
Conjunctival Manifestations of Systemic Diseases
Practice Questions
Cicatricial Conjunctival Disorders
Practice Questions
Pterygium and Pinguecula
Practice Questions
Conjunctival Trauma
Practice Questions
Subconjunctival Hemorrhage
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app