
Diseases of the Conjunctiva — MCQs

On this page
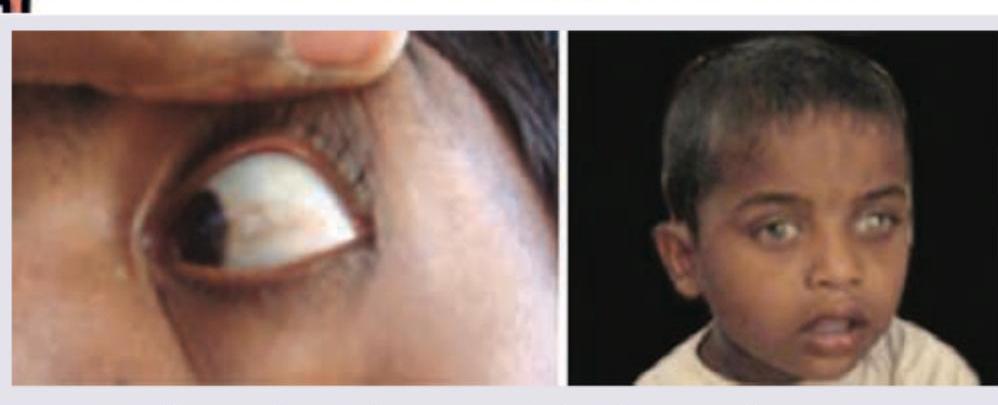
All are true about the image shown EXCEPT:
Spring catarrh is a type of conjunctivitis caused by
All are true about Vernal conjunctivitis EXCEPT:
All of the following are causes of acute red eye EXCEPT:
Identify the diagnosis based on the clinical image shown.

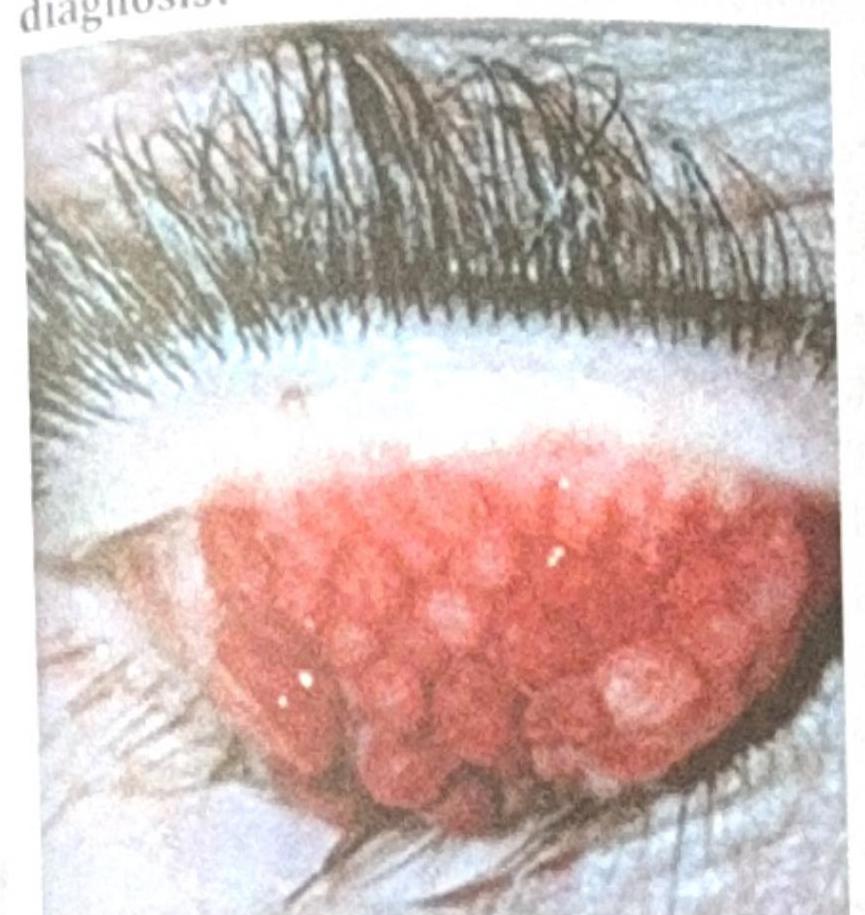
A patient with contact lens use for the past 2 years presents with lens intolerance, ropy discharge without seasonal variation, and the ocular findings shown in the image below. What is the most probable diagnosis?
Identify the correct sequence of staining in dry eyes? 1. Fluorescein stain 2. Lissamine green 3. Rose Bengal stain
Which of the following is true about pterygium?
Herbert's pits are seen in:
NOT a feature of trachoma:
Practice by Chapter
Conjunctivitis: Bacterial
Practice Questions
Conjunctivitis: Viral
Practice Questions
Conjunctivitis: Allergic
Practice Questions
Conjunctivitis: Chronic
Practice Questions
Degenerations of Conjunctiva
Practice Questions
Benign Tumors of Conjunctiva
Practice Questions
Malignant Tumors of Conjunctiva
Practice Questions
Conjunctival Manifestations of Systemic Diseases
Practice Questions
Cicatricial Conjunctival Disorders
Practice Questions
Pterygium and Pinguecula
Practice Questions
Conjunctival Trauma
Practice Questions
Subconjunctival Hemorrhage
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app