
Diseases of the Conjunctiva — MCQs

On this page
A patient from a rural, resource-limited community presents with chronic redness and discharge from the eye for several months. On examination, eversion of the upper eyelid reveals the conjunctival findings shown in the image. What is the most likely diagnosis?

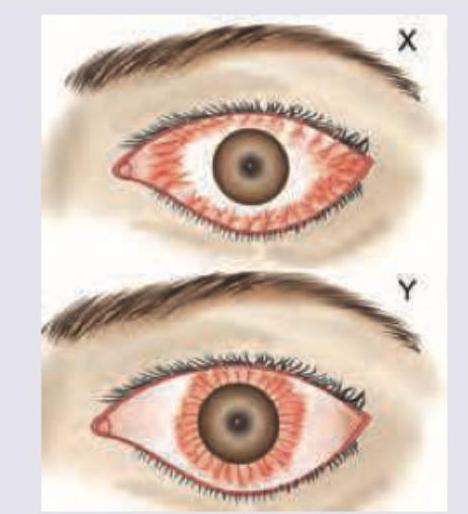
A 22-year-old Air-force test pilot presents after flying a sortie. Eye examination shows:
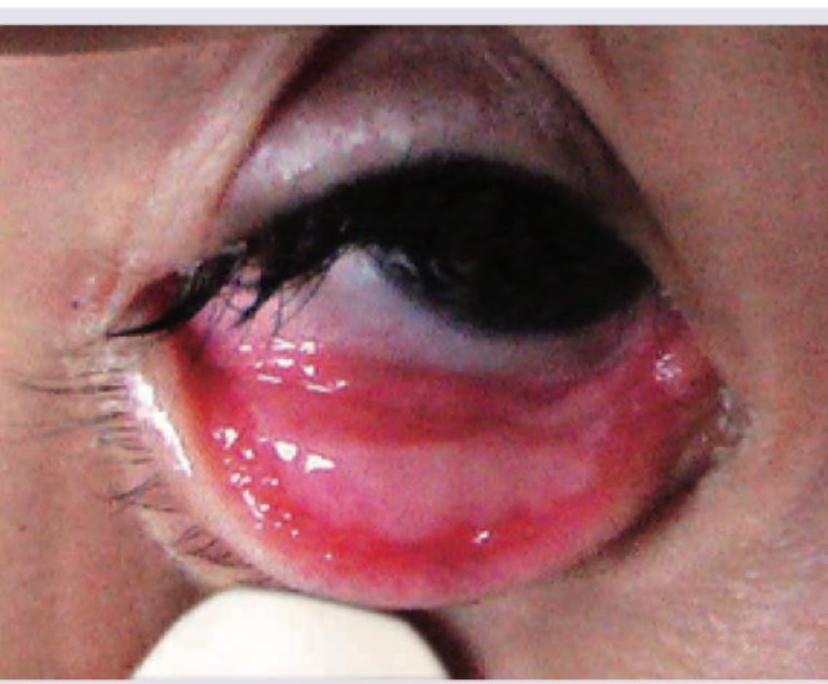
What is correct about the image shown below?
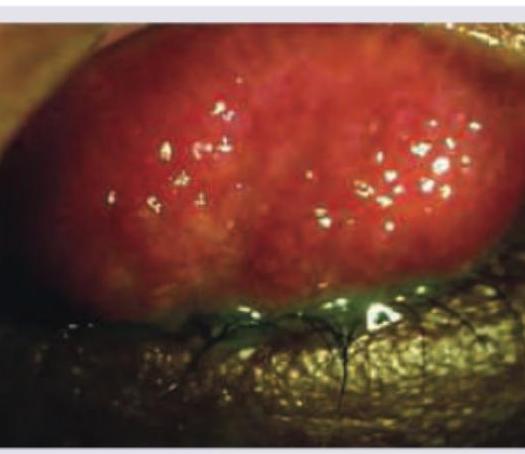
A patient from slum presents with grittiness in eyes. Everted eyelid shows: (Recent NEET Pattern 2016-17)

A 5-year-old child presents with severe itching and ropy discharge. Image shows:

The image shown below depicts:

A five-year-old child presents with recurrent episodes of thick, woody pseudomembranous growths on the conjunctiva that have been difficult to remove. Which condition is shown in the image below?
A 25-year-old lady presents with itching and excoriation of the skin near inner canthus bilaterally. Sometimes a slight mucopurulent discharge is present in the morning. What is the best treatment for this patient? (Recent NEET Pattern 2016-17)
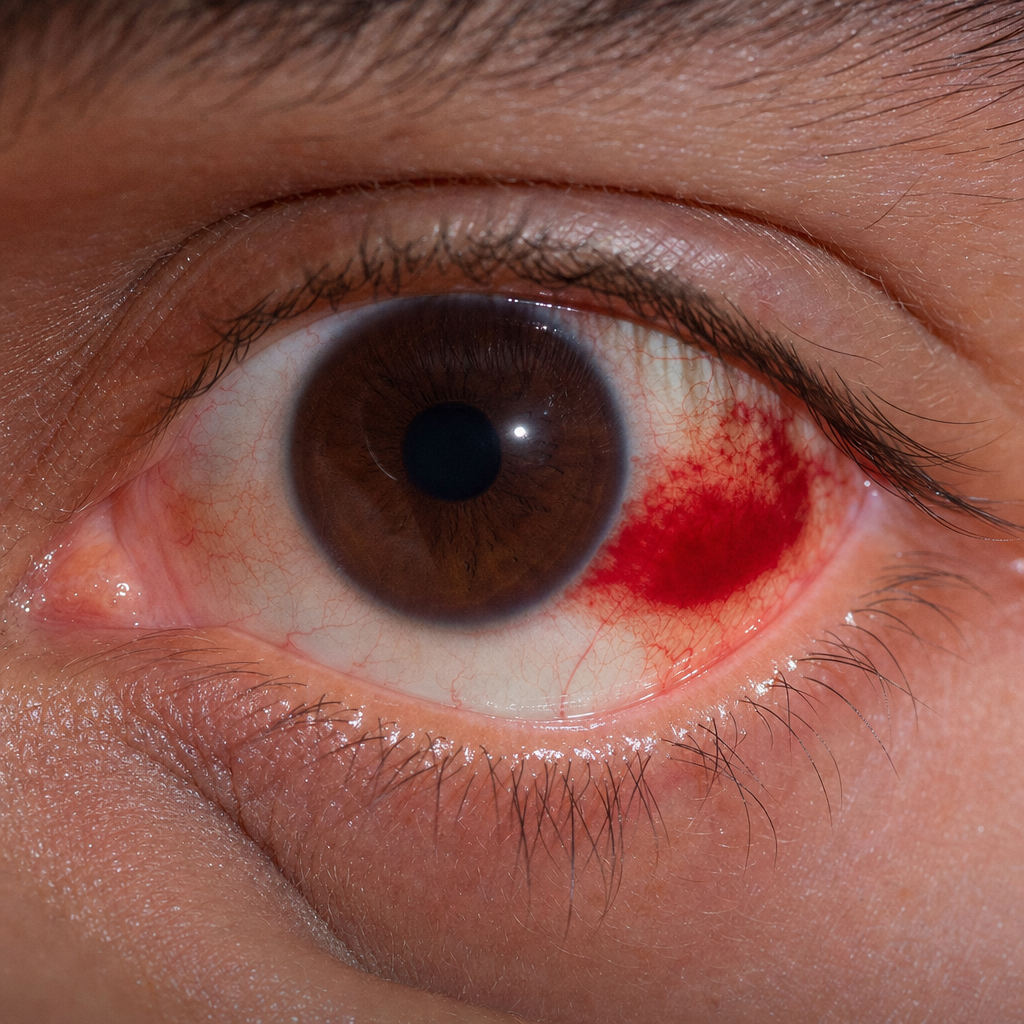
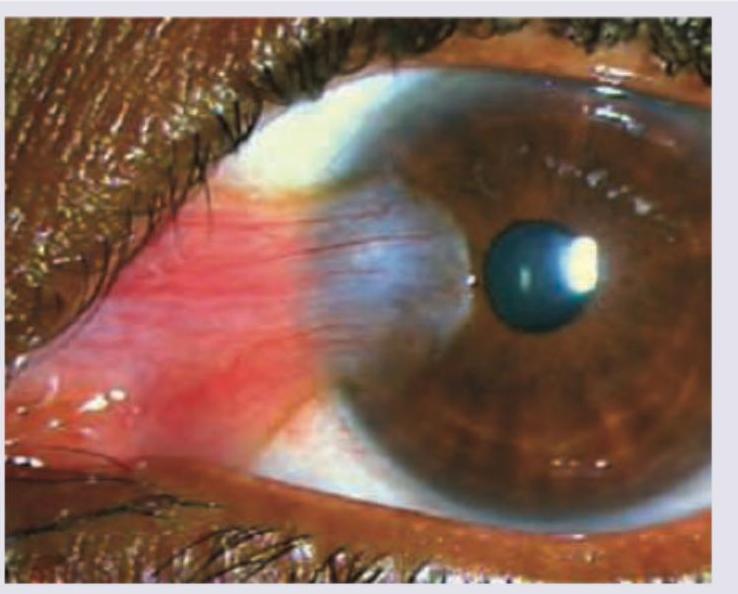
A patient presents with red eye. What is correct about the image shown below?
All are correct about the lesion shown except:
Practice by Chapter
Conjunctivitis: Bacterial
Practice Questions
Conjunctivitis: Viral
Practice Questions
Conjunctivitis: Allergic
Practice Questions
Conjunctivitis: Chronic
Practice Questions
Degenerations of Conjunctiva
Practice Questions
Benign Tumors of Conjunctiva
Practice Questions
Malignant Tumors of Conjunctiva
Practice Questions
Conjunctival Manifestations of Systemic Diseases
Practice Questions
Cicatricial Conjunctival Disorders
Practice Questions
Pterygium and Pinguecula
Practice Questions
Conjunctival Trauma
Practice Questions
Subconjunctival Hemorrhage
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app