
Diseases of the Conjunctiva — MCQs

On this page
According to WHO, which method is applied for prophylactic use in ophthalmia neonatorum?
A swimmer presents with redness and mucopurulent discharge after exiting a swimming pool. There is no history of contact lens wear, and examination reveals no corneal involvement. What is the probable diagnosis?
Which of the following is NOT a feature of allergic conjunctivitis?
Viral Conjunctivitis is most commonly caused by which virus?
Trantas spots are seen in which of the following conditions?
Which of the following are features of vernal keratoconjunctivitis?
What is the dosage of retinol palmitate for early stages of xerophthalmia?
A patient with a history of recurrent trachomatous infection presents with the ocular finding shown in the image. Arlt's lines are also noted on eversion of the upper eyelid. Identify the ocular condition shown in the image.
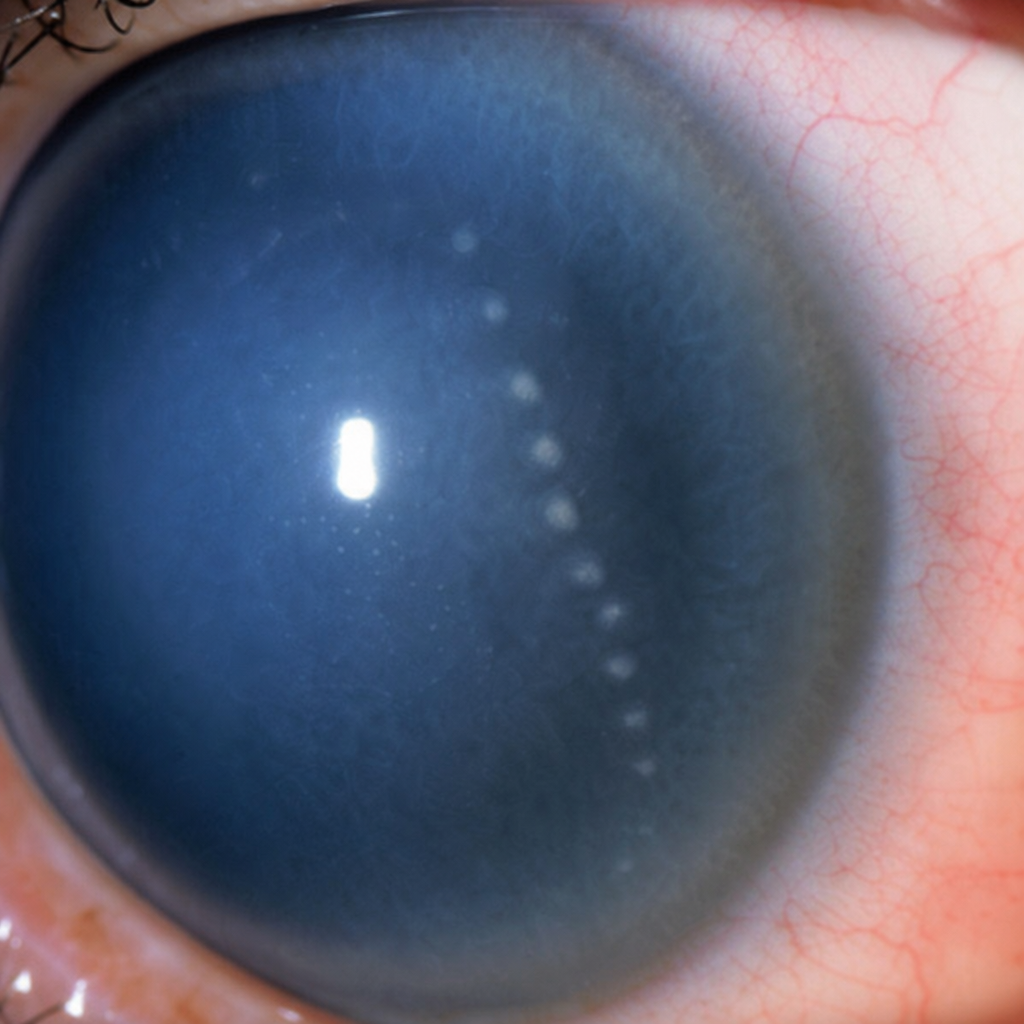
The finding seen in the image is:
A 10-year-old boy presents with severe itching in both eyes, photophobia, and a recurrent seasonal worsening of symptoms every summer. What is the diagnosis shown in the image?

Practice by Chapter
Conjunctivitis: Bacterial
Practice Questions
Conjunctivitis: Viral
Practice Questions
Conjunctivitis: Allergic
Practice Questions
Conjunctivitis: Chronic
Practice Questions
Degenerations of Conjunctiva
Practice Questions
Benign Tumors of Conjunctiva
Practice Questions
Malignant Tumors of Conjunctiva
Practice Questions
Conjunctival Manifestations of Systemic Diseases
Practice Questions
Cicatricial Conjunctival Disorders
Practice Questions
Pterygium and Pinguecula
Practice Questions
Conjunctival Trauma
Practice Questions
Subconjunctival Hemorrhage
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app