
Diseases of the Conjunctiva — MCQs

On this page
Cicatrising trachoma is seen in which stage?
Which of the following is NOT true regarding epidemic keratoconjunctivitis?
Arlt's line is seen in which condition?
What is the drug of choice for Spring Catarrh?
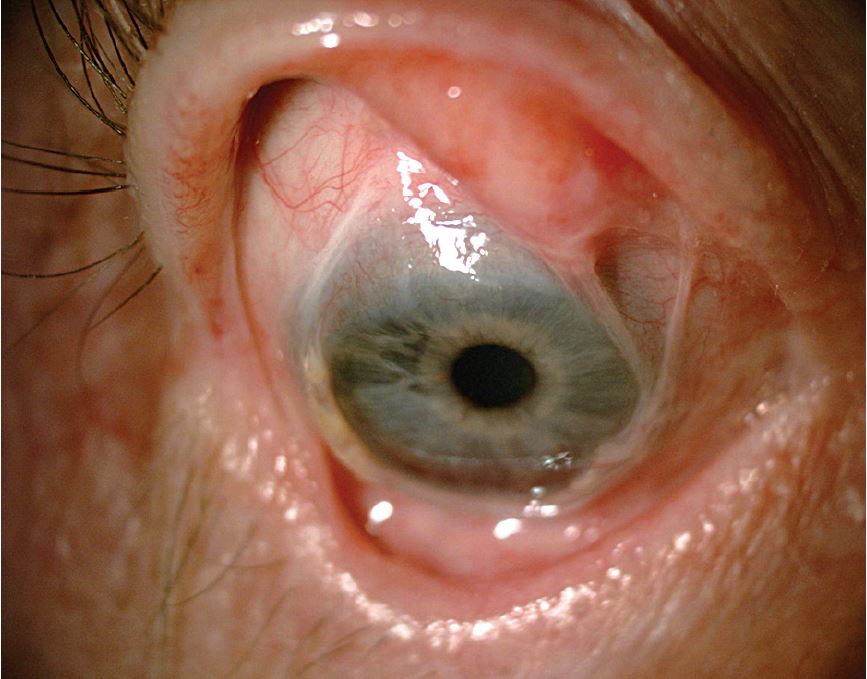
Diagnosis of the given condition is:
A 7-year-old patient presents with a conjunctival nodule, with a history of previous TB treatment. The nodule has now encroached onto the limbus. What is the most likely diagnosis?
Ophthalmia nodosa is seen with which of the following conditions?
Conjunctiva in vitamin A deficiency shows which of the following changes?
Follicle formation may be seen in all of the following except?
What is the most common malignant cancer of the conjunctiva?
Practice by Chapter
Conjunctivitis: Bacterial
Practice Questions
Conjunctivitis: Viral
Practice Questions
Conjunctivitis: Allergic
Practice Questions
Conjunctivitis: Chronic
Practice Questions
Degenerations of Conjunctiva
Practice Questions
Benign Tumors of Conjunctiva
Practice Questions
Malignant Tumors of Conjunctiva
Practice Questions
Conjunctival Manifestations of Systemic Diseases
Practice Questions
Cicatricial Conjunctival Disorders
Practice Questions
Pterygium and Pinguecula
Practice Questions
Conjunctival Trauma
Practice Questions
Subconjunctival Hemorrhage
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app