
Degenerations of Conjunctiva — MCQs

Phlyctenular conjunctivitis is primarily associated with hypersensitivity to which of the following?
Which of the following statements about pterygium is false?
Stocker's line is seen in?
Perforating injuries with retained intraocular foreign body are more serious than those without because of:
Statement 1 - A 59-year-old patient presents with flaccid bullae. Histopathology shows a suprabasal acantholytic split. Statement 2 - The row of tombstones appearance is diagnostic of Pemphigus vulgaris.
Koeppe nodules are typically found on which part of the eye?
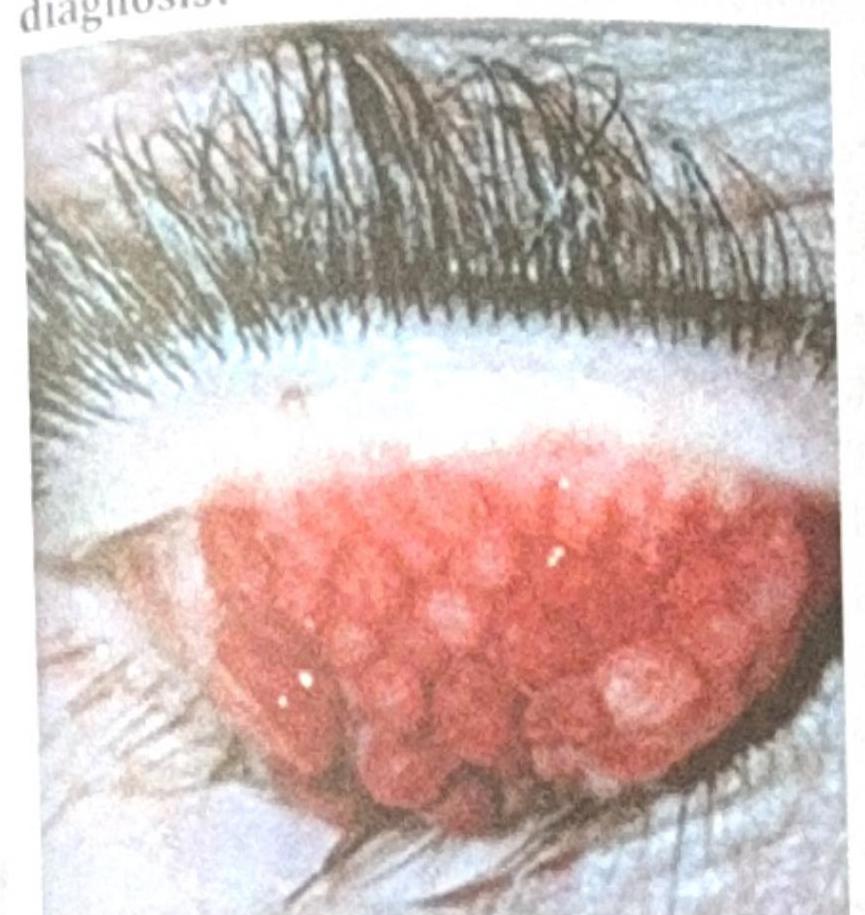
A patient with contact lens use for the past 2 years presents with the ocular findings shown in the image below. What is the most probable diagnosis?
Features of vernal conjunctivitis are:
Epithelial xerosis of conjunctiva is caused by?
NOT a feature of trachoma:
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app