
Conjunctivitis: Chronic — MCQs

Which of the following findings is typically NOT seen in a patient with allergic conjunctivitis?
A 25-year-old male presents with recurrent bilateral conjunctival hyperemia and a gritty sensation. Likely diagnosis?
Arlt's line is seen in?
Phlyctenular conjunctivitis is primarily associated with hypersensitivity to which of the following?
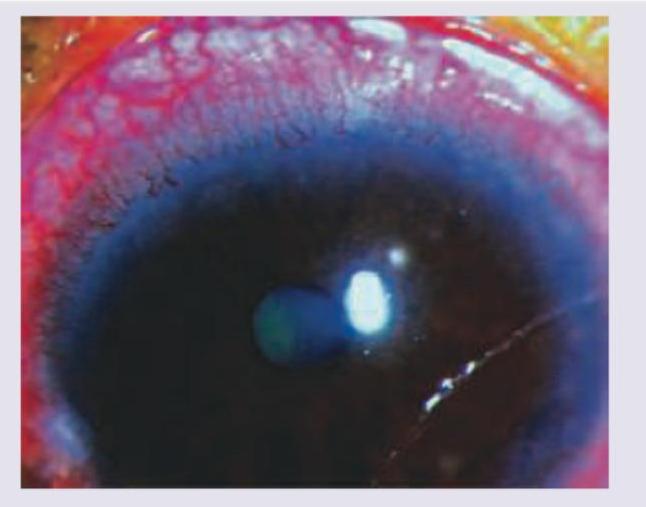
Identify the diagnosis based on the clinical image shown.

Which of the following is not a treatment option for vernal keratoconjunctivitis?
Inclusion conjunctivitis is caused by:
Features of vernal conjunctivitis are:
Unilateral frontal blisters with upper lid edema and conjunctivitis is seen in?
What does the following image show?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app