
Diseases of the Conjunctiva — MCQs

On this page
Image-based question: Diagnosis is:
A 52-year-old male outdoor worker presents with a fleshy growth in his left eye associated with foreign body sensation and redness for 3 years. On examination, a triangular fibrovascular tissue is seen arising from the nasal conjunctiva and encroaching 3 mm onto the cornea, crossing the pupillary axis. Best-corrected visual acuity is reduced to 6/18, and keratometry reveals significant with-the-rule astigmatism. There is no evidence of active inflammation. What is the most appropriate management for this patient?
Best treatment for a small boy with itching in summers and Horner-Trantas spots:
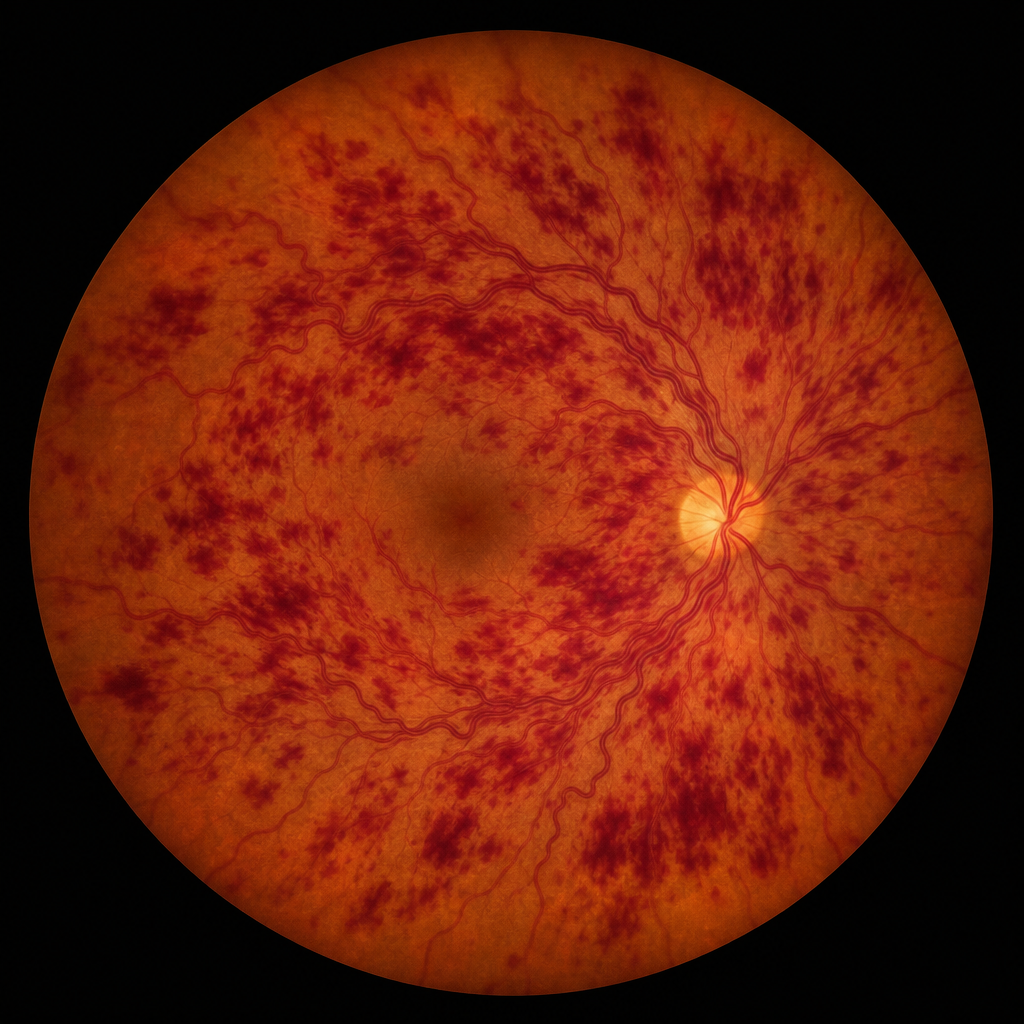
A 58-year-old hypertensive woman presents with sudden painless loss of vision in her left eye noticed on waking. Her blood pressure is 168/96 mmHg. There is no relative afferent pupillary defect. The fundus photograph of the left eye shows diffuse venous tortuosity and widespread retinal hemorrhages in all four quadrants, consistent with central retinal vein occlusion (Image 3). Which of the following investigations is most important to guide immediate management and reduce the risk of neovascular complications?
Which of the following statements regarding acute conjunctivitis is FALSE?
Condition in which the eyelid is adhered to the conjunctiva is:
Giant papillary conjunctivitis is most commonly seen in association with which of the following?
What is the specific topical remedy suggested for angular conjunctivitis?
Which of the following are features of vernal conjunctivitis?
Which of the following is NOT a sequela of trachoma?
Practice by Chapter
Conjunctivitis: Bacterial
Practice Questions
Conjunctivitis: Viral
Practice Questions
Conjunctivitis: Allergic
Practice Questions
Conjunctivitis: Chronic
Practice Questions
Degenerations of Conjunctiva
Practice Questions
Benign Tumors of Conjunctiva
Practice Questions
Malignant Tumors of Conjunctiva
Practice Questions
Conjunctival Manifestations of Systemic Diseases
Practice Questions
Cicatricial Conjunctival Disorders
Practice Questions
Pterygium and Pinguecula
Practice Questions
Conjunctival Trauma
Practice Questions
Subconjunctival Hemorrhage
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app