
Specialty Contact Lenses — MCQs

Which of the following is not a feature of keratoconus?
Keratometry is useful in measuring:
Acute corneal hydrops is seen in:
Which is an emergency therapeutic indication of keratoplasty?
Assertion: Myopia is a risk factor for retinal detachment. Reason: In myopia, the axial length of the eye increases, causing the retina to thin and become more prone to detachment.
Which of the following is a true statement regarding the human eye?
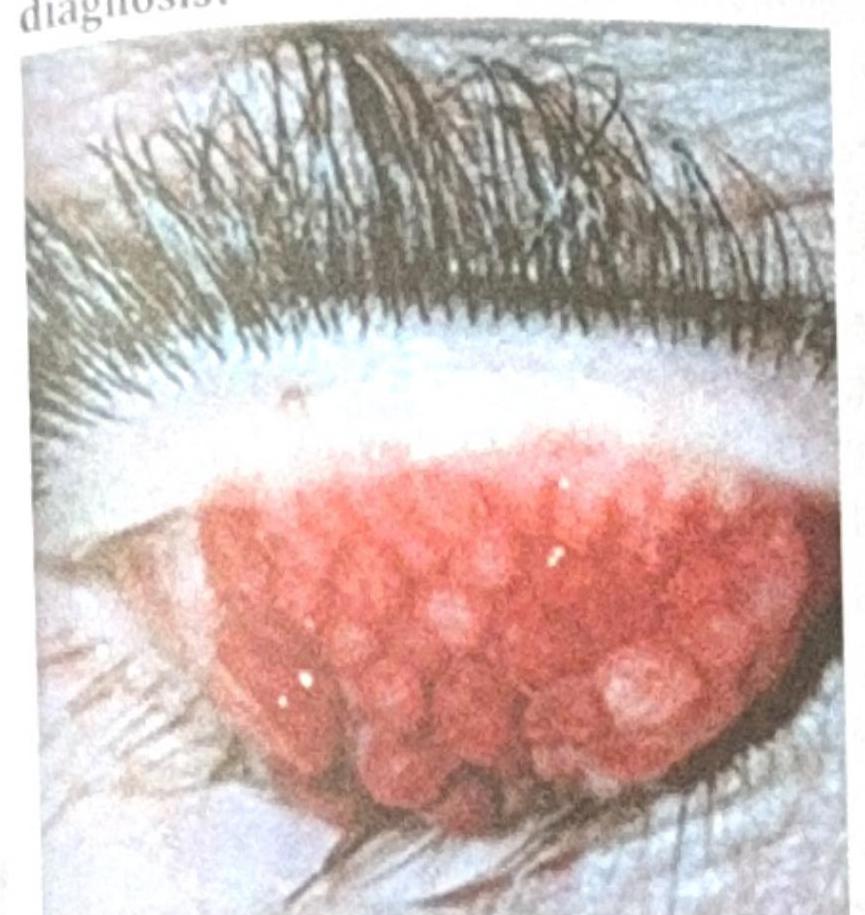
A patient with contact lens use for the past 2 years presents with the ocular findings shown in the image below. What is the most probable diagnosis?
What is the minimum contact period required for effective chlorination of drinking water?
A 23-year-old woman is diagnosed with chlamydia. Her partner refuses testing. What contact tracing approach is most appropriate?
Shortening of 2 mm of axial length of the eyeball causes?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app