
Contact Lens — MCQs

On this page
Recovery in cataract surgery is fastest with which of the following techniques?
What is the equatorial diameter of the lens?
In which of the following uveitic conditions is it contraindicated to implant an intraocular lens after cataract extraction?
What is the best method to prevent infection after cataract surgery?
What causes a 'Rosette cataract'?
Lens develops from which germ layer?
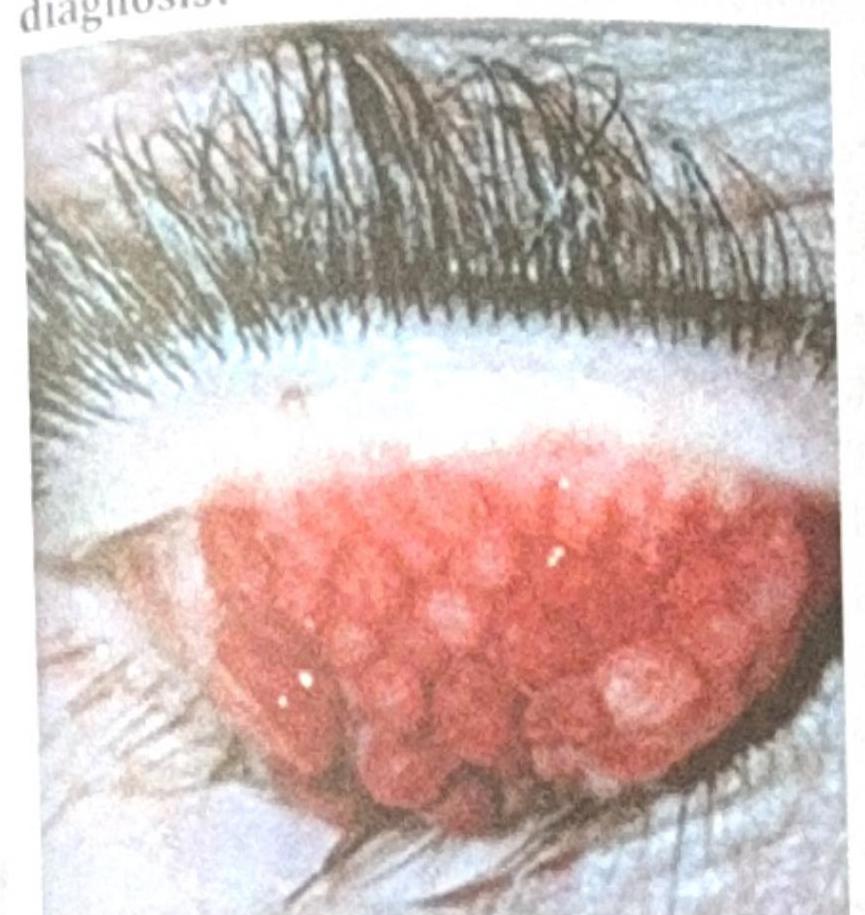
A patient with contact lens use for the past 2 years presents with the ocular findings shown in the image below. What is the most probable diagnosis?
Which of the following is an advantage of contact lenses over normal glasses?
Rigid gas permeable (RGP) lenses are made from which of the following combinations of materials?
What is the most common infection in contact lens users?
Practice by Chapter
Contact Lens Materials
Practice Questions
Soft Contact Lenses
Practice Questions
Rigid Gas Permeable Lenses
Practice Questions
Specialty Contact Lenses
Practice Questions
Contact Lens Fitting Principles
Practice Questions
Contact Lens Care and Maintenance
Practice Questions
Contact Lens Complications
Practice Questions
Contact Lenses for Keratoconus
Practice Questions
Orthokeratology
Practice Questions
Contact Lenses for Astigmatism
Practice Questions
Contact Lenses for Presbyopia
Practice Questions
Scleral Contact Lenses
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app