
Screening Programs — MCQs

Which of the following is NOT a core component of the WHO's global STI control strategy?
Specificity of a diagnostic test is defined as:
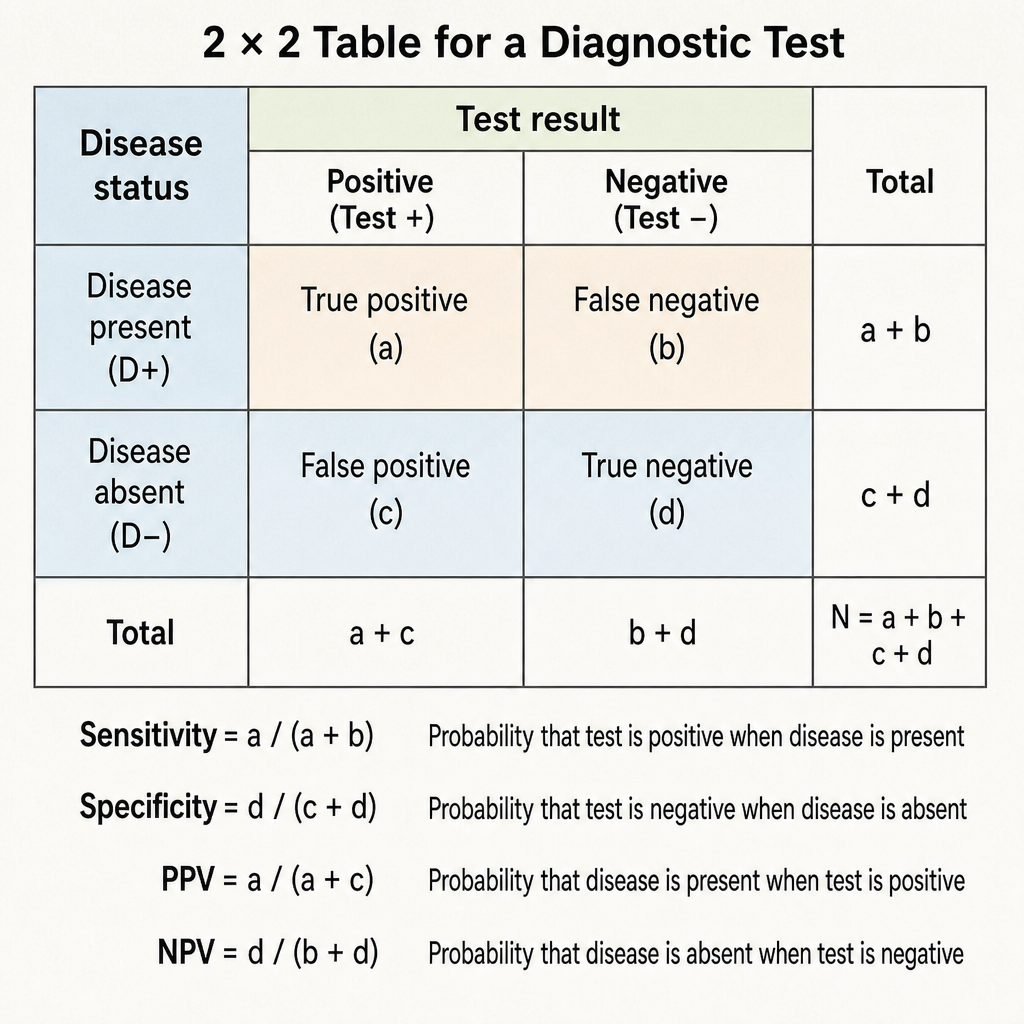
What is the correct formula for calculating the positive predictive value (PPV) of a screening test?
Under NPCB, screening of school children is first done by -
Which measure indicates the diagnostic power of a test to correctly identify those with a disease?
Which of the following procedures is not typically covered by the National Programme for Control of Blindness (NPCB) for reimbursement of surgery done by a non-governmental organization (NGO) eye hospital?
All of the following are the targets for National Programme for Control of Blindness (NPCB), EXCEPT:
Which of the following is a true statement about screening tests for genetic diseases?
In primary open-angle glaucoma (POAG), which of the following findings is NOT typically seen?
What is the gold standard method for visualizing the periphery of the retina?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app