
Basic Sciences as Related to Eye — MCQs

On this page
The visual axis of the eye meets the retina at a point which:
What is the normal ratio of the diameter of a retinal arteriole to a retinal venule?
What is the primary function of the superior oblique muscle?
Which muscle is the primary intorter of the eye?
Aqueous flare seen in the anterior chamber is due to:
Coloboma of the iris is defined as:
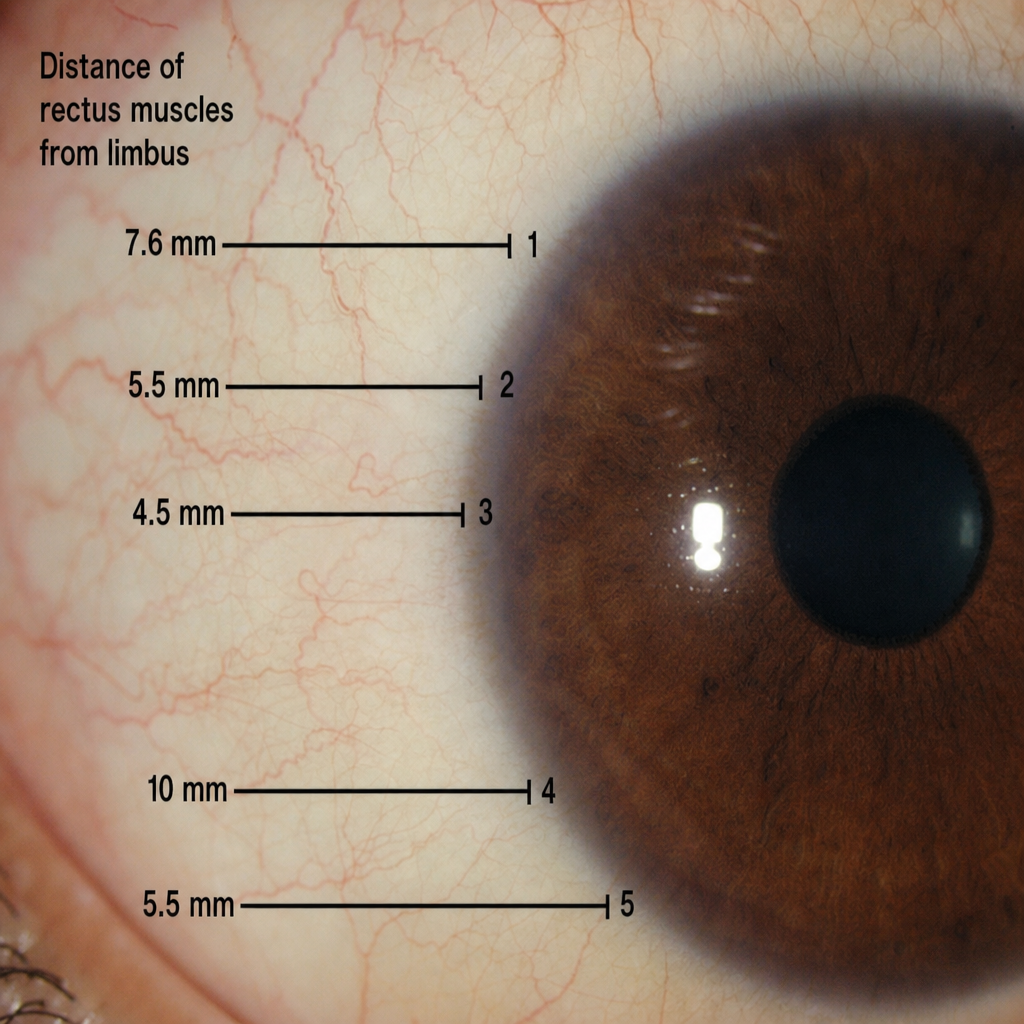
What is the distance of Muscle 5 from the limbus?
Amsler's sign is seen in which of the following conditions?
Mucopolysaccharide hyaluronic acid is present in which of the following ocular structures?
Which of the following is seen in non-granulomatous uveitis?
Practice by Chapter
Embryology of Eye
Practice Questions
Ocular Anatomy
Practice Questions
Ocular Physiology
Practice Questions
Ocular Biochemistry
Practice Questions
Ocular Microbiology
Practice Questions
Ocular Pharmacology
Practice Questions
Ocular Pathology
Practice Questions
Ocular Genetics
Practice Questions
Ocular Immunology
Practice Questions
Visual Neuroscience
Practice Questions
Ocular Imaging Physics
Practice Questions
Laser Physics in Ophthalmology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app