
Basic Sciences as Related to Eye — MCQs

On this page
At what age does tear production typically begin in a child?
What is the most common type of ocular lymphoma?
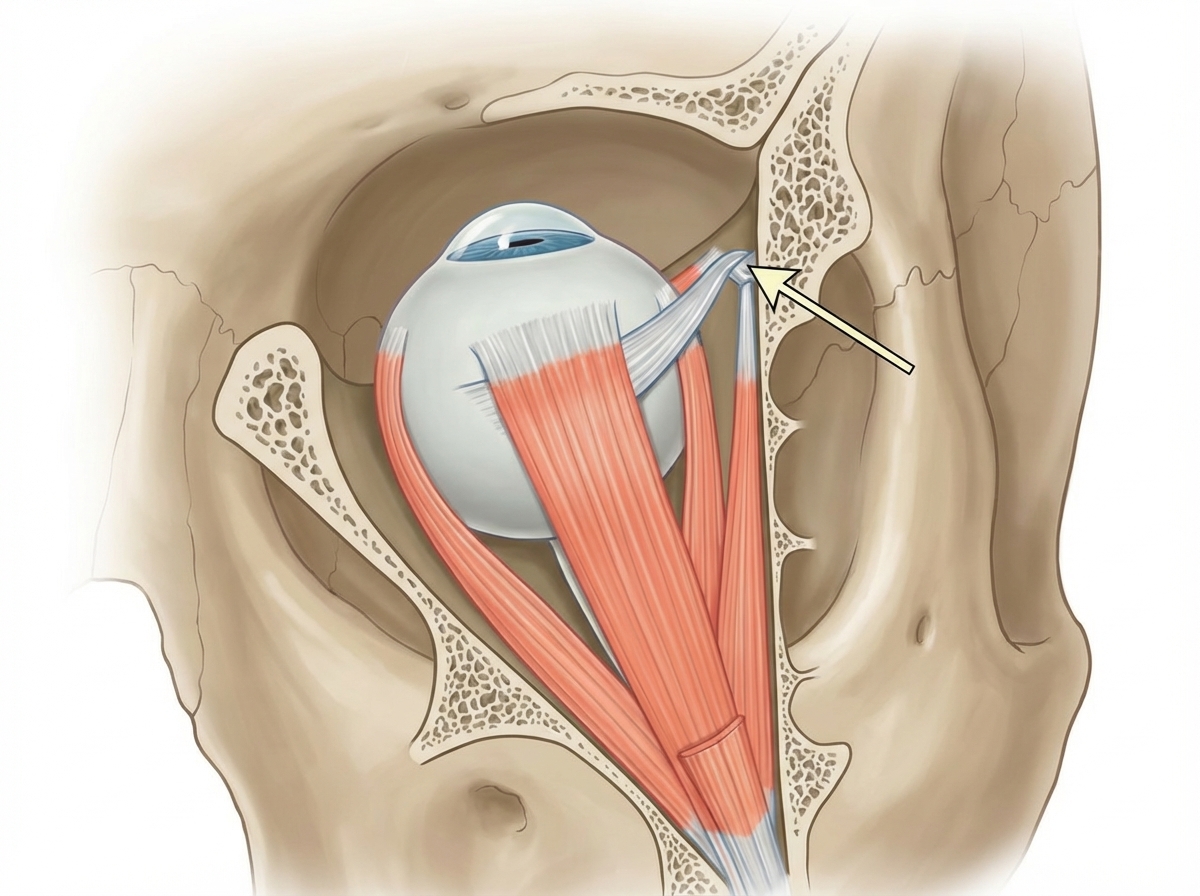
The arrow points towards which anatomical structure?
Normal aqueous production rate is about:
The electroretinogram may assist in the diagnosis of all of the following, except:
What is the most common etiological variety of uveitis?
Which of the following statements about the depth of the anterior chamber is FALSE?
What is the Zonula of Zinn?
Which is the thinnest layer of the tear film?
Which of the following actions is NOT caused by the superior oblique muscle?
Practice by Chapter
Embryology of Eye
Practice Questions
Ocular Anatomy
Practice Questions
Ocular Physiology
Practice Questions
Ocular Biochemistry
Practice Questions
Ocular Microbiology
Practice Questions
Ocular Pharmacology
Practice Questions
Ocular Pathology
Practice Questions
Ocular Genetics
Practice Questions
Ocular Immunology
Practice Questions
Visual Neuroscience
Practice Questions
Ocular Imaging Physics
Practice Questions
Laser Physics in Ophthalmology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app