
Basic Sciences as Related to Eye — MCQs

On this page
Which of the following muscles does not originate from the orbital apex?
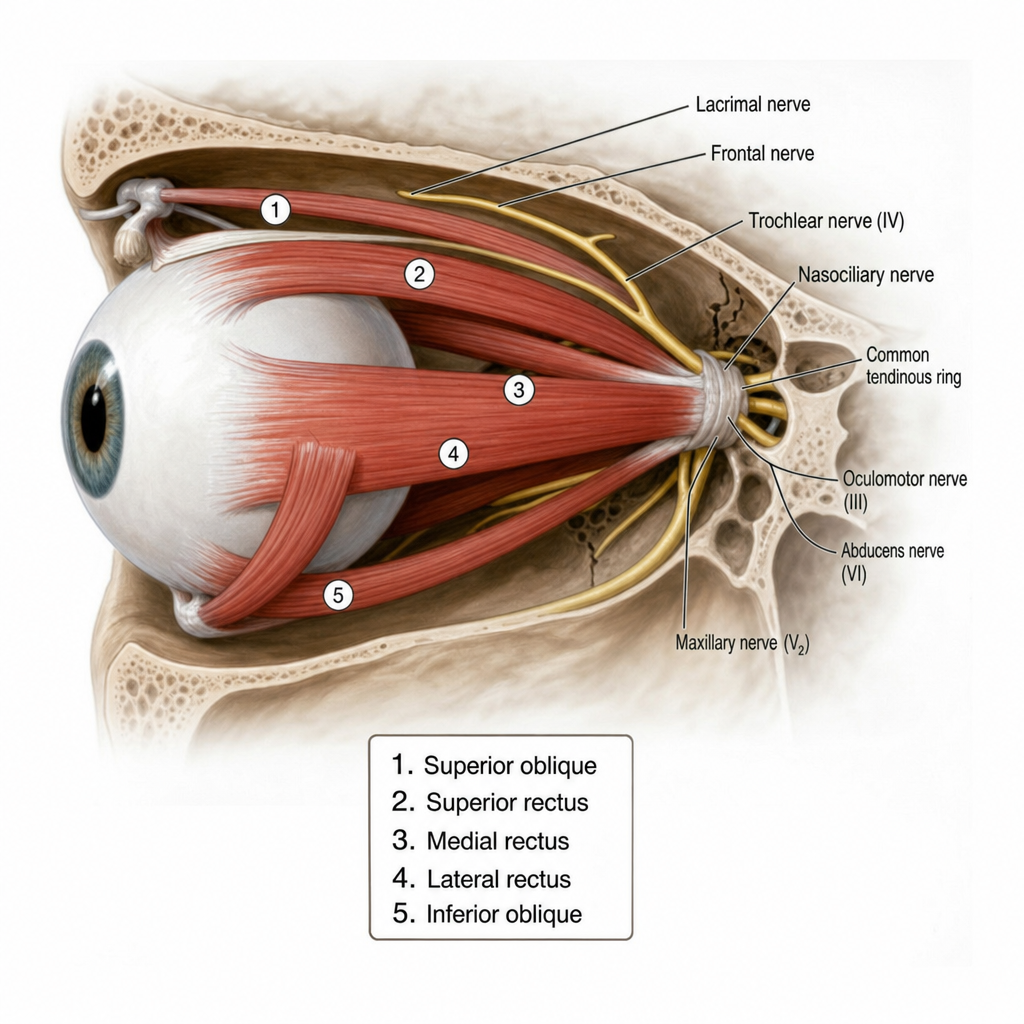
The posterior end of which muscle insertion lies near the macula?
Vascular invasion is commonly seen in which of the following ocular tumors?
Which of the following will block the ionic pump in the corneal endothelium necessary for maintaining corneal deturgescence and transparency?
A person has defective blue color appreciation. What is the best name for this condition?
What is the approximate size of the optic disc in millimeters?
Henle's layer refers to the thickened outer plexiform layer in the region of what part of the retina?
Coloured halos are seen in all conditions listed below, except –
What is the distance from the sclerocorneal junction to the insertion of the medial rectus muscle on the sclera?
What are isochromatic charts used for?
Practice by Chapter
Embryology of Eye
Practice Questions
Ocular Anatomy
Practice Questions
Ocular Physiology
Practice Questions
Ocular Biochemistry
Practice Questions
Ocular Microbiology
Practice Questions
Ocular Pharmacology
Practice Questions
Ocular Pathology
Practice Questions
Ocular Genetics
Practice Questions
Ocular Immunology
Practice Questions
Visual Neuroscience
Practice Questions
Ocular Imaging Physics
Practice Questions
Laser Physics in Ophthalmology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app