
Basic Sciences as Related to Eye — MCQs

On this page
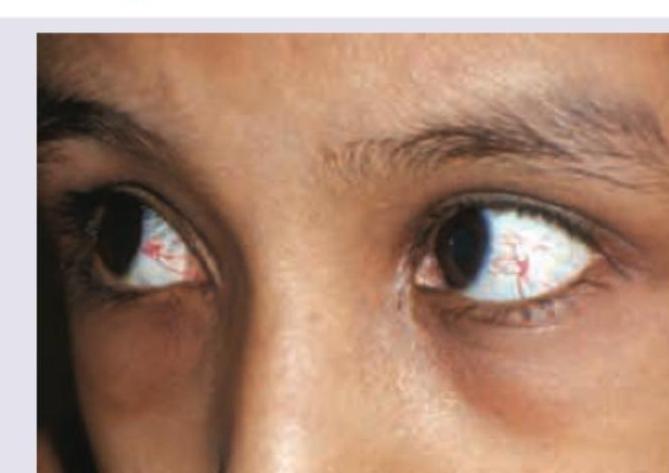
The image shows a child with?
Father of ophthalmology?
Which of the following is known as the dangerous zone of the eye?
Depth of anterior chamber (AC) is:
Which ocular structure is the most radiosensitive?
Which of the following statements about vitreous is false?
Which mode of ultrasonography is used to measure the axial length of the eyeball?
Muscae volitantes is seen in?
What is the normal aqueous production rate in the human eye?
Which of the following is a specific sign of albinism?
Practice by Chapter
Embryology of Eye
Practice Questions
Ocular Anatomy
Practice Questions
Ocular Physiology
Practice Questions
Ocular Biochemistry
Practice Questions
Ocular Microbiology
Practice Questions
Ocular Pharmacology
Practice Questions
Ocular Pathology
Practice Questions
Ocular Genetics
Practice Questions
Ocular Immunology
Practice Questions
Visual Neuroscience
Practice Questions
Ocular Imaging Physics
Practice Questions
Laser Physics in Ophthalmology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app