
Basic Sciences as Related to Eye — MCQs

On this page
Visual acuity is a measure of:
Light entering the eye passes through which retinal layer first?
Synchysis refers to
A 52-year-old man presents with painless, gradual vision loss in his right eye over two hours. He has a history of myocardial infarction and takes aspirin daily. The physical examination reveals no vision in the right eye. At the molecular level, which of the following components is essential for the first step of the visual cascade?
Which is the longest and thinnest extraocular muscle?
All statements are true about the eye of a newborn except?
In near vision, what change occurs in the eye?
A person with defective blue color appreciation is called?
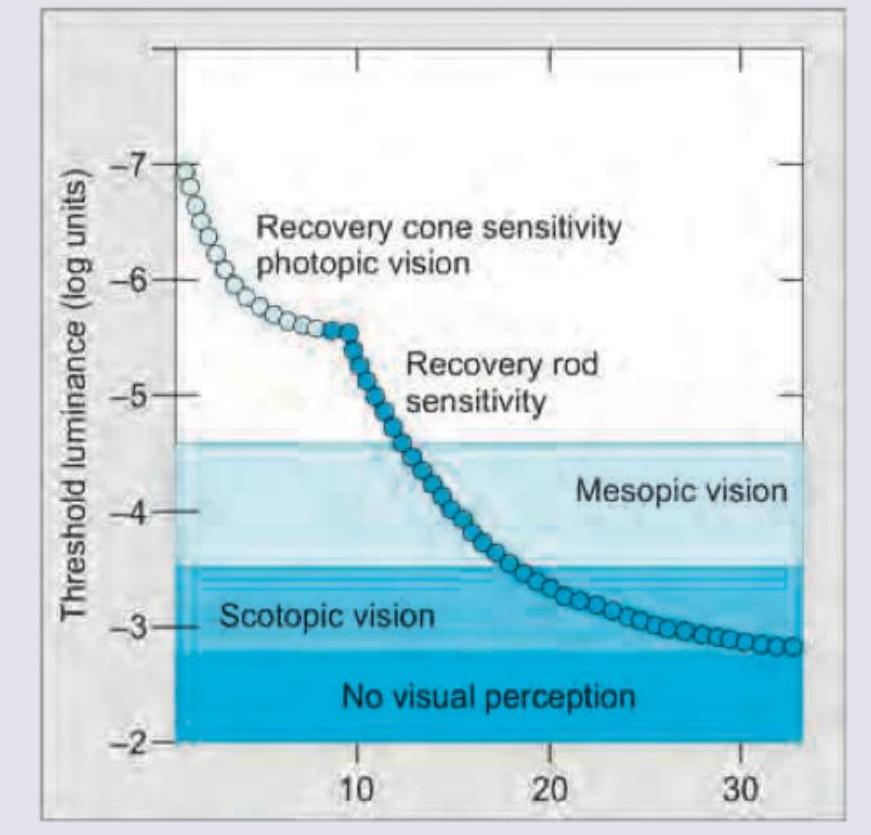
All of the following are correct about the image shown except: (Recent NEET Pattern 2016-17)

The image given below shows:
Practice by Chapter
Embryology of Eye
Practice Questions
Ocular Anatomy
Practice Questions
Ocular Physiology
Practice Questions
Ocular Biochemistry
Practice Questions
Ocular Microbiology
Practice Questions
Ocular Pharmacology
Practice Questions
Ocular Pathology
Practice Questions
Ocular Genetics
Practice Questions
Ocular Immunology
Practice Questions
Visual Neuroscience
Practice Questions
Ocular Imaging Physics
Practice Questions
Laser Physics in Ophthalmology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app