
Basic Sciences as Related to Eye — MCQs

On this page
Which of the following correctly describes the changes that take place during dark adaptation? A) Retinol is converted to vitamin D B) Dilated pupils C) Eyes sensitive to light D) Functional rhodopsin is formed (Opsin binds with 11-cis-retinal)
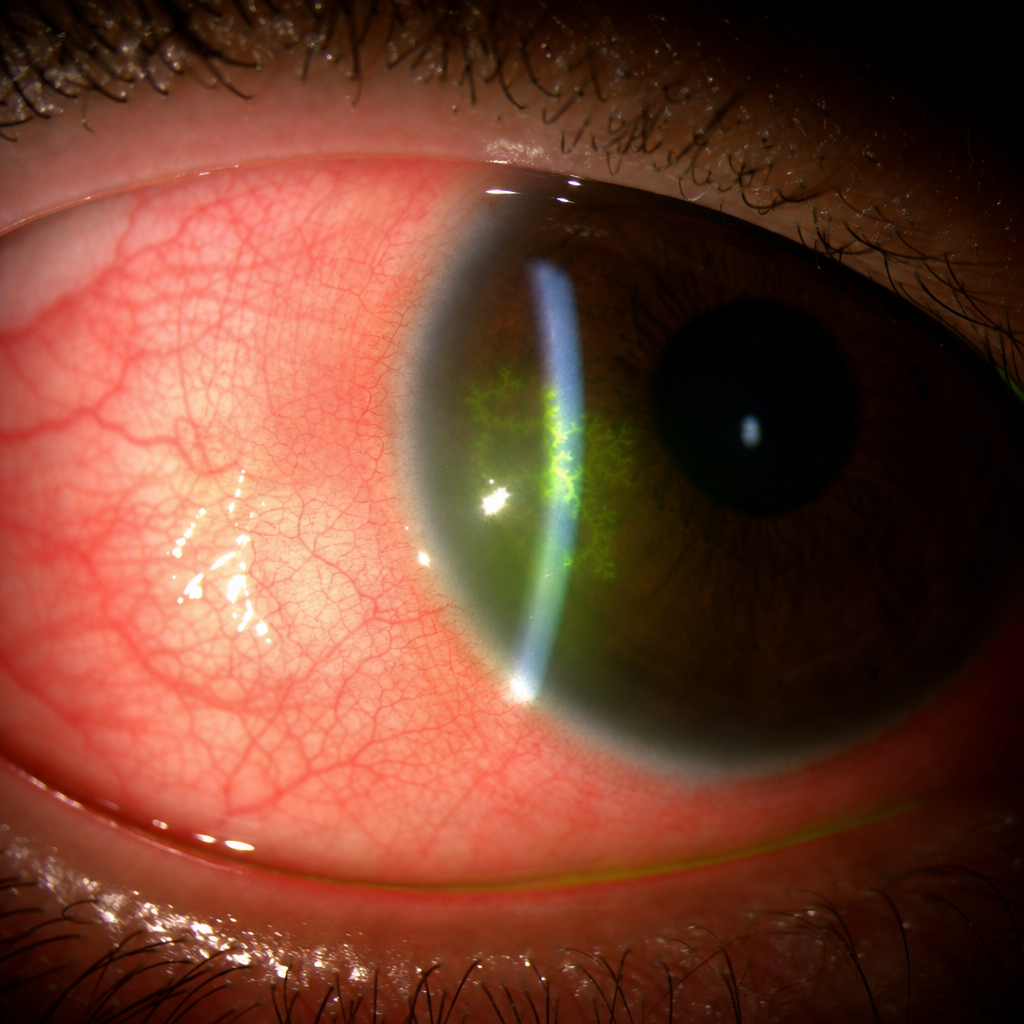
A 34-year-old woman presents with a 3-day history of unilateral redness, photophobia, and foreign body sensation in the right eye. She reports a similar episode two years ago that resolved with eye drops. Her visual acuity is 6/12 in the affected eye. There is no history of contact lens use. The slit-lamp examination is shown in Image 1. Which of the following is the most appropriate first-line treatment?
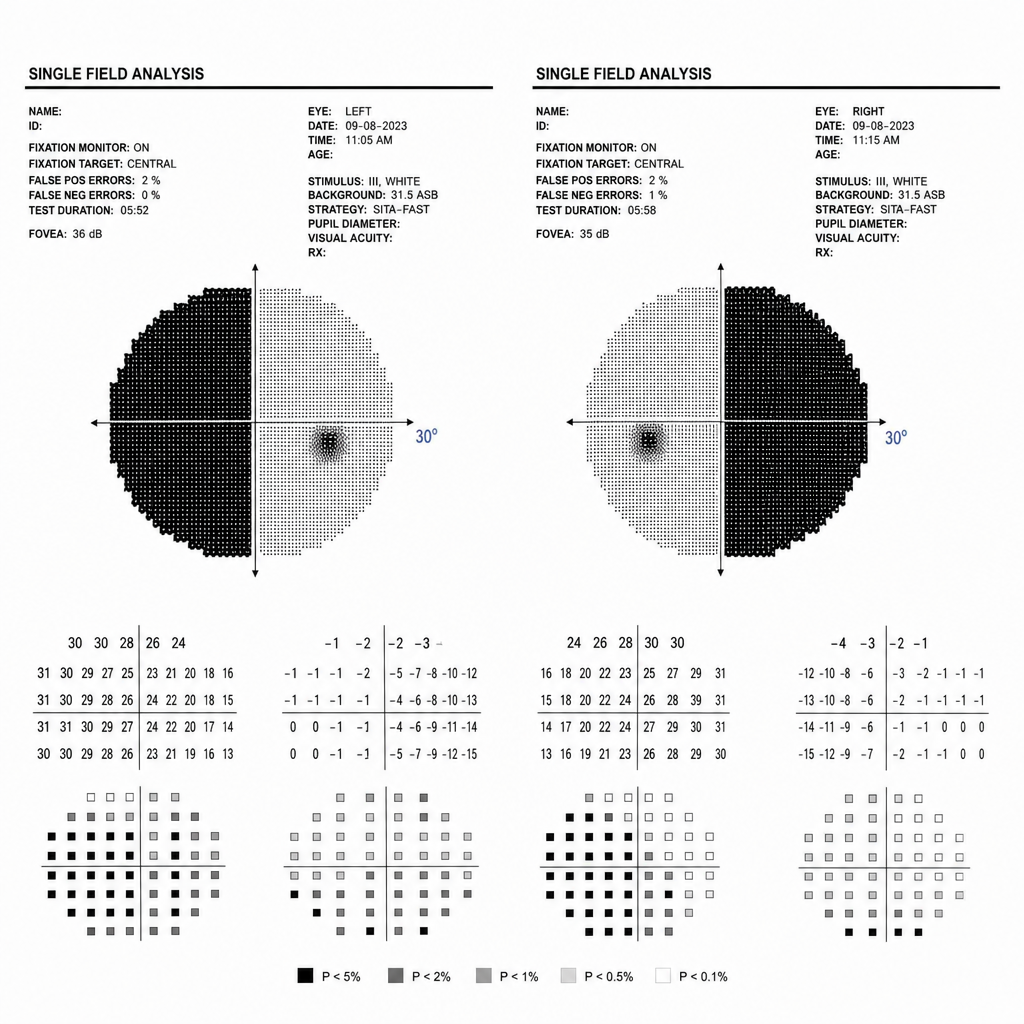
A 45-year-old woman presents with a 6-month history of gradually worsening peripheral vision and two episodes of headache. She also reports secondary amenorrhoea and galactorrhoea. Her visual field chart is shown (Image 1). Which anatomical structure is most likely being compressed to produce this pattern of visual loss?
A point that falls on the horopter excites which of the following?
The aqueous flare is best demonstrated by which instrument?
Maximum density of goblet cells is seen in which part of the conjunctiva?
In ERG, 'A' waves correspond to which structures?
Aqueous humor is produced by which structure?
The ducts of the main lacrimal gland open into which part of the conjunctival sac?
What is the blood supply of the prelaminar optic nerve?
Practice by Chapter
Embryology of Eye
Practice Questions
Ocular Anatomy
Practice Questions
Ocular Physiology
Practice Questions
Ocular Biochemistry
Practice Questions
Ocular Microbiology
Practice Questions
Ocular Pharmacology
Practice Questions
Ocular Pathology
Practice Questions
Ocular Genetics
Practice Questions
Ocular Immunology
Practice Questions
Visual Neuroscience
Practice Questions
Ocular Imaging Physics
Practice Questions
Laser Physics in Ophthalmology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app