
Rectocele and Enterocele — MCQs

Injury to which of the following muscles that forms the deep support of the perineal body causes cystocele, enterocele and urethral descent?
Which of the following is not felt with a digital rectal examination?
All are causes of prolapse of cervix EXCEPT:
Which of the following is not a perineal approach for the condition shown in the image?

What is the treatment for uterine prolapse in nulliparous women?
In gonorrhea, which is not a presenting feature?
What is the last resort treatment for rectal prolapse in childhood?
Not a feature of rectosigmoid endometriosis on MRI
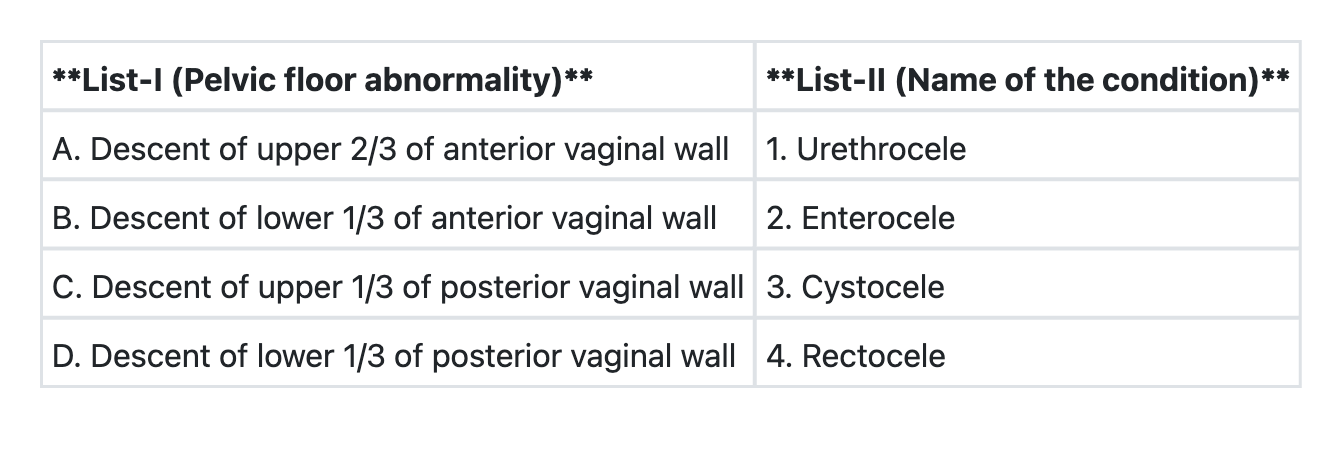
Match List-I with List-II and select the correct answer using the code given below the Lists:
Moschcowitz repair is done for:
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app