
Urogynecology — MCQs

On this page
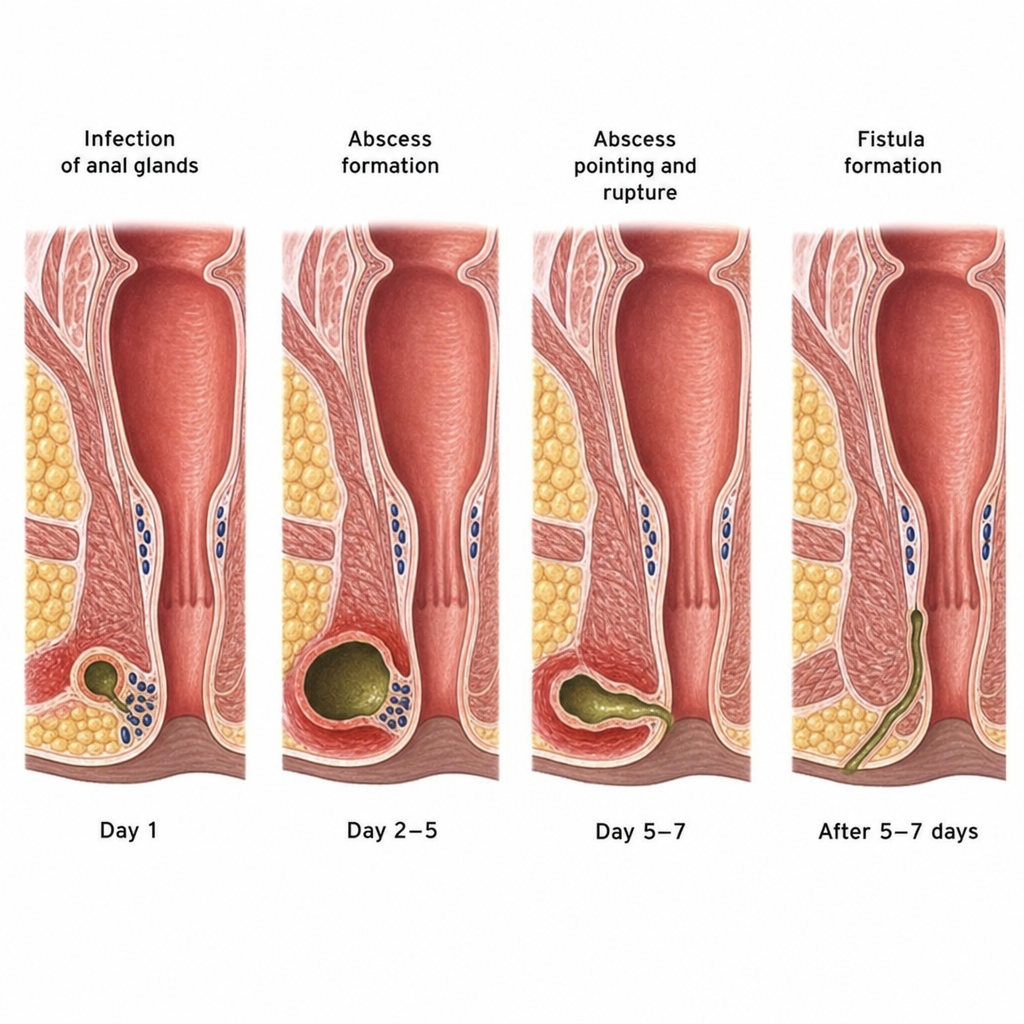
Fistula formation due to the stated etiology occurs within what timeframe?
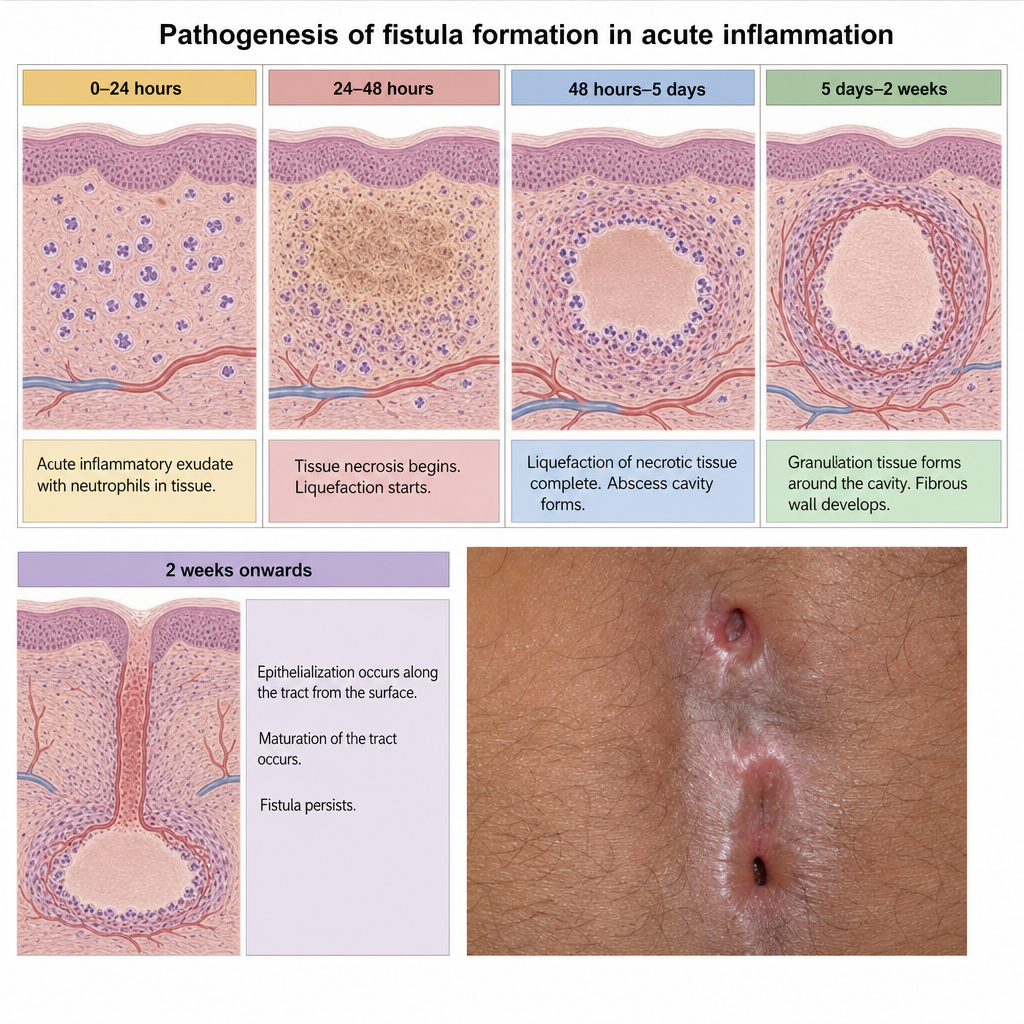
Fistula formation due to the stated etiology following prolonged obstructed labor occurs within what timeframe?
What is the commonest site of surgical uretero-vaginal fistula?
A woman had a difficult labour. She complains of dribbling of urine 7 days after delivery. What is the diagnosis?
Which of the following is the most common site for genito-urinary fistula?
Which of the following are criteria for opting Le Fort's operation for surgical correction of pelvic organ prolapse? I. Procidentia in old age II. Unfit for long duration surgery III. Associated uterine pathology IV. Coital function no longer required Select the correct answer using the code given below :
Which of the following is measured without any straining while examination under POP-Q system?
Surgical treatment by 'ventrosuspension of uterus' is used for what condition ?
Vesicovaginal fistula is classified as complicated if it has which of the following features ? 1. Size - more than 3 cm 2. Bladder involvement - Trigonal/Juxta-urethral 3. Location - Midvaginal 4. Presence of prior radiation Select the correct answer using the code given below :
Which of the following are essential steps of Fothergill's operation? 1. Laparoscopic or vaginal ligation 2. Amputation of cervix 3. Plication of Mackenrodt's ligaments in front of cervix 4. Anterior colporrhaphy Select the correct answer using the code given below.
Practice by Chapter
Pelvic Floor Anatomy and Function
Practice Questions
Urinary Incontinence: Classification
Practice Questions
Stress Urinary Incontinence
Practice Questions
Overactive Bladder and Urge Incontinence
Practice Questions
Pelvic Organ Prolapse: Classification
Practice Questions
Cystocele and Urethrocele
Practice Questions
Uterine Prolapse
Practice Questions
Rectocele and Enterocele
Practice Questions
Surgical Management in Urogynecology
Practice Questions
Conservative Management Approaches
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app