
Urogynecology — MCQs

On this page
Childbirth trauma leading to urinary incontinence is seen least in females with which type of pelvis?
All of the following are abdominal sling surgeries done for uterine preservation in patients of uterine prolapse, EXCEPT?
A patient who has undergone Fothergill's repair for uterine prolapse may experience which of the following complications, except?
What is the treatment of choice for second-degree uterine prolapse in a 24-year-old nulliparous woman?
In the immediate postoperative period following a hysterectomy, a patient develops leakage of urine. What is the most likely cause?
What is the most important structure preventing uterine prolapse?
A 55-year-old woman presents with chronic pelvic discomfort, lower back pain, constipation, difficulty with walking, and impaired coitus. Pelvic examination reveals that the uterine cervix lies low within the vaginal canal but does not protrude through the introitus. For minor degrees of this condition, Kegel exercises are sometimes prescribed. How are Kegel exercises performed?
What is the best treatment for severe stress incontinence without prolapse?
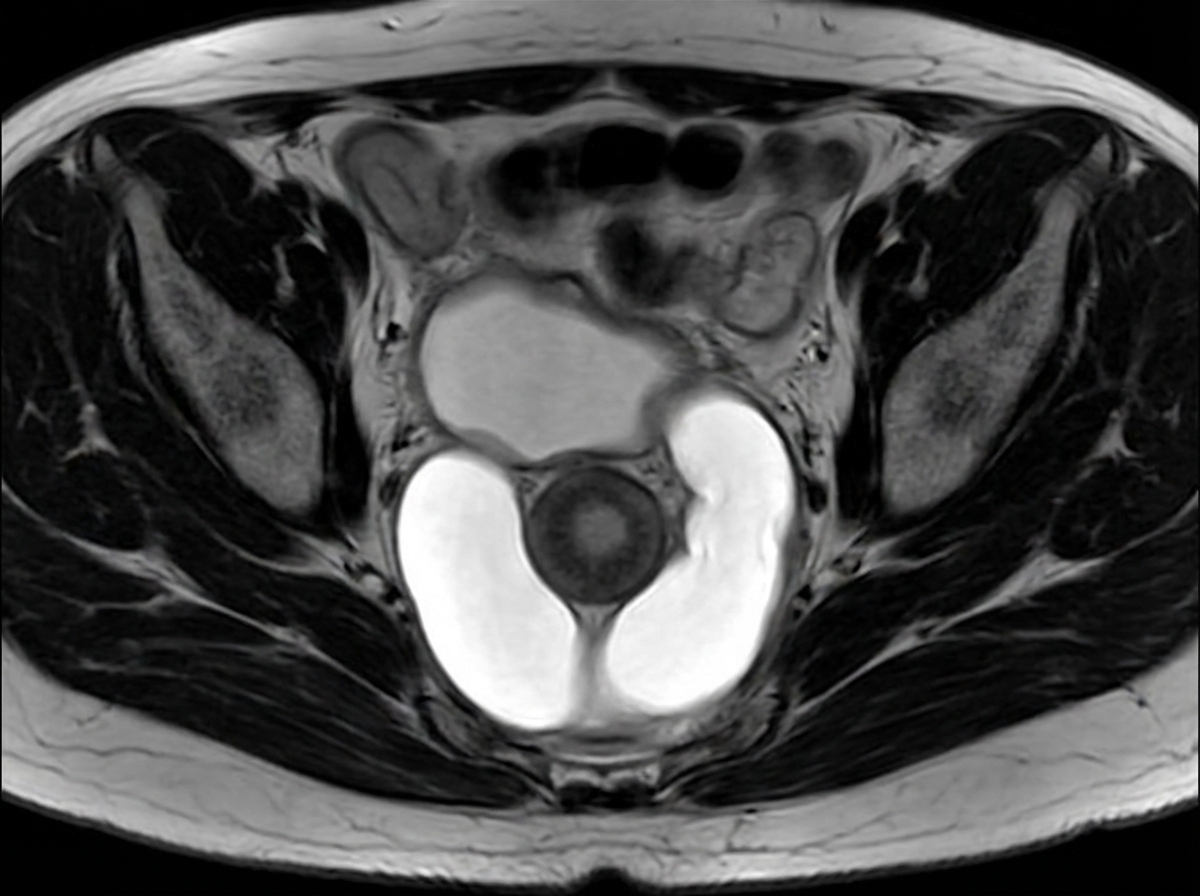
A female patient presents with post-void dribbling, recurrent urinary tract infections, and a tender anterior vaginal wall mass. Her MRI pelvis is shown in the image. What is the most likely diagnosis?
What is the treatment for genuine stress incontinence?
Practice by Chapter
Pelvic Floor Anatomy and Function
Practice Questions
Urinary Incontinence: Classification
Practice Questions
Stress Urinary Incontinence
Practice Questions
Overactive Bladder and Urge Incontinence
Practice Questions
Pelvic Organ Prolapse: Classification
Practice Questions
Cystocele and Urethrocele
Practice Questions
Uterine Prolapse
Practice Questions
Rectocele and Enterocele
Practice Questions
Surgical Management in Urogynecology
Practice Questions
Conservative Management Approaches
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app