
Urogynecology — MCQs

On this page
With reference to the displacement of uterus, the treatment of choice for genuine stress urinary incontinence is:
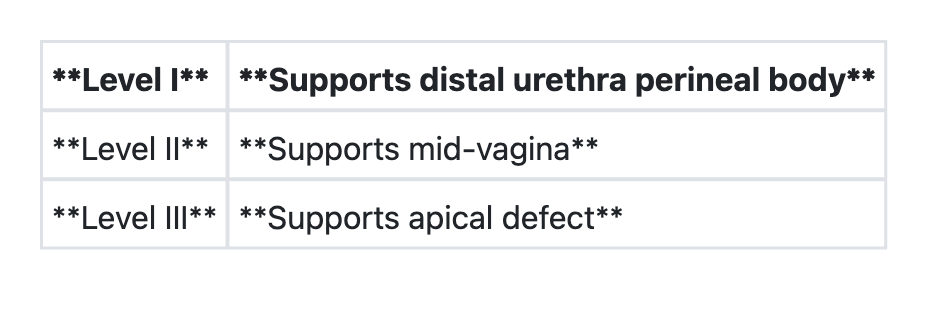
Regarding 'DeLancey's levels of vaginal support', consider the following pairs:
A 40 year old lady is examined and found to have uterovaginal prolapse. What is the appropriate surgery to prevent recurrence?
Which of the following is NOT a component of Fothergill’s operation as a conservative surgery for uterovaginal prolapse?
The level of external cervical os in a second degree utero vaginal prolapse is:
Treatment of choice in 28 year old nullipara with third degree cervical descent is:
Surgical treatment of choice for a 20 year old nulliparous woman with uterine prolapse is:
Which of the following is NOT an ideally suited condition for use of ring pessary in case of uterine prolapse?
Which of the following symptoms can be associated with pelvic organ prolapse? 1. Difficulty in passing urine 2. Incomplete evacuation of urine 3. Urgency and frequency Select the correct answer using the code given below:
A 30-year-old female, G2L2, with a history of cervical elongation presents for surgical consultation. What is the surgery of choice?
Practice by Chapter
Pelvic Floor Anatomy and Function
Practice Questions
Urinary Incontinence: Classification
Practice Questions
Stress Urinary Incontinence
Practice Questions
Overactive Bladder and Urge Incontinence
Practice Questions
Pelvic Organ Prolapse: Classification
Practice Questions
Cystocele and Urethrocele
Practice Questions
Uterine Prolapse
Practice Questions
Rectocele and Enterocele
Practice Questions
Surgical Management in Urogynecology
Practice Questions
Conservative Management Approaches
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app