
Urogynecology — MCQs

On this page
Which of the following are correct regarding pathology of stress urinary incontinence? 1. Hypermobility of urethra 2. Descent of bladder neck and proximal urethra below pelvic diaphragm 3. Lowered urethral pressure 4. Increased detrusor activity
The reference point 'zero' in POPQ (Pelvic Organ Prolapse Quantification) classification is taken as
What is the most common cause of vault prolapse following hysterectomy ?
What is the commonest cause of Vulvo-Vaginal Fistula in developing countries ?
A woman who is being investigated for infertility is diagnosed to have a nulliparous prolapse of the uterus. The most appropriate management will be
Which of the following are the features of backache due to genital prolapse? 1. The pain is experienced on getting up in the morning. 2. The patient complains of a diffuse pain over the sacrum. 3. There is no local tenderness. 4. The pain occurs more commonly among multiparous than nulliparous women. Select the correct answer using the code given below:
A 20-year-old young woman, who was delivered two months ago at home by a nurse, presents with a complaint of something protruding through the vulva. The clinical examination reveals a cystocele, rectocele, and the cervix 1 cm above the introitus. The most appropriate management will be
A parous woman notices a bulge at the vulva that diminishes in size following micturition. She also finds it difficult to initiate micturition. What is the likely diagnosis ?
A woman of child-bearing age develops a second-degree uterine prolapse with supravaginal elongation of the cervix. What will be the most appropriate management?
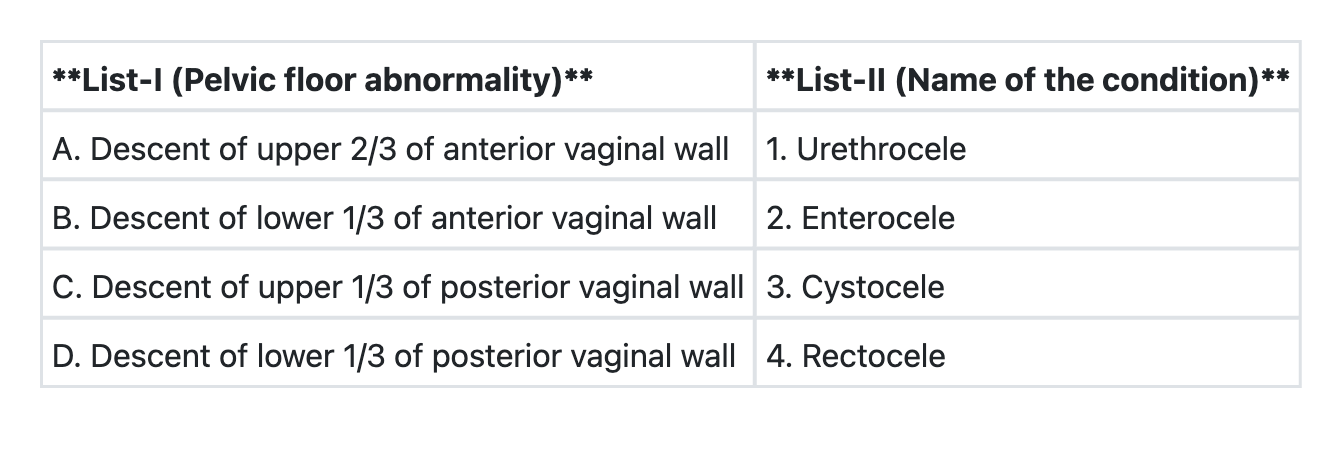
Match List-I with List-II and select the correct answer using the code given below the Lists:
Practice by Chapter
Pelvic Floor Anatomy and Function
Practice Questions
Urinary Incontinence: Classification
Practice Questions
Stress Urinary Incontinence
Practice Questions
Overactive Bladder and Urge Incontinence
Practice Questions
Pelvic Organ Prolapse: Classification
Practice Questions
Cystocele and Urethrocele
Practice Questions
Uterine Prolapse
Practice Questions
Rectocele and Enterocele
Practice Questions
Surgical Management in Urogynecology
Practice Questions
Conservative Management Approaches
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app