
Reproductive Endocrinology — MCQs

On this page
Which of the following is NOT a typical symptom or sign of Polycystic Ovarian Disease (PCOD)?
All of the following statements about Androgen Insensitivity Syndrome are true except?
Determination of serum progesterone level to document ovulation. For the evaluation, select the most appropriate day of a normal 28-day menstrual cycle for a woman with 5-day menstrual periods.
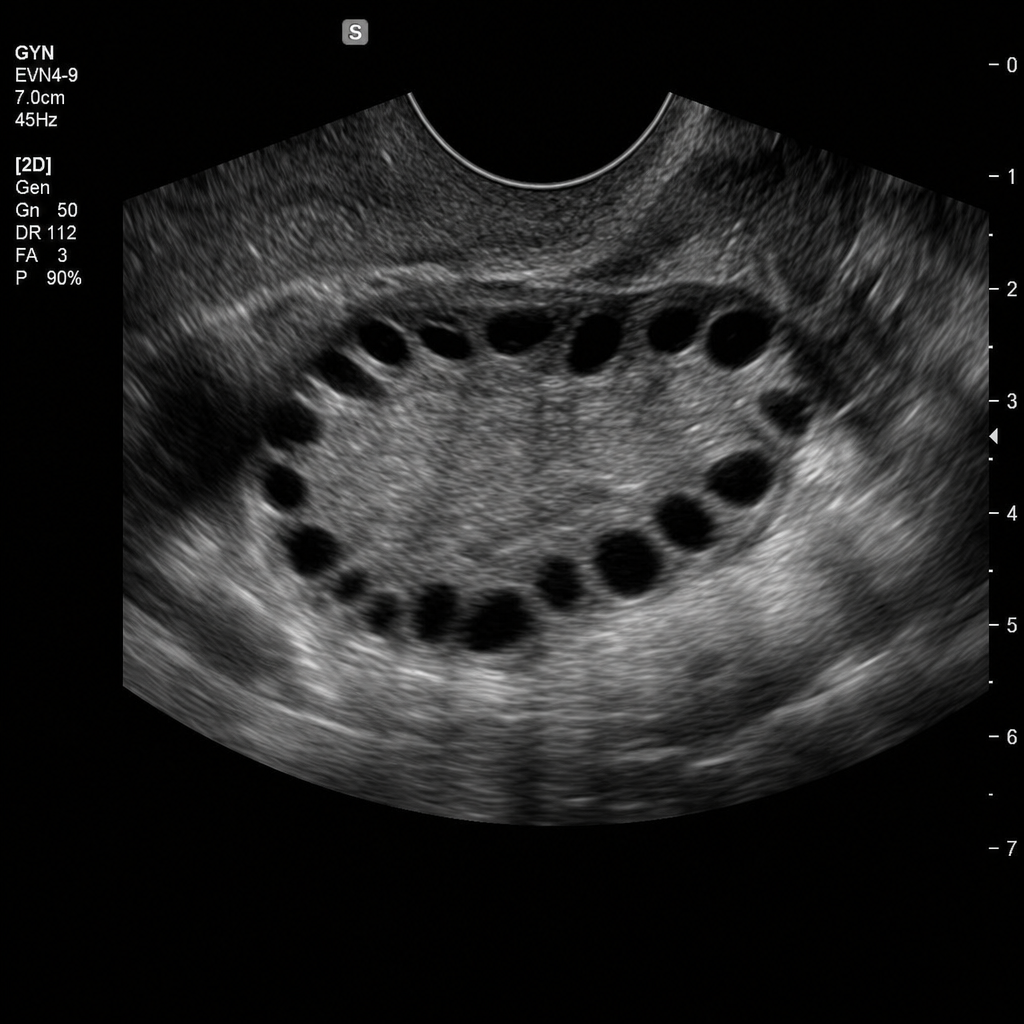
A patient presents with a history of amenorrhea and hirsutism. Ultrasound of the ovary is provided. What is the most likely diagnosis?
A 16-year-old female has not yet started having menstrual cycles. Her secondary sex characteristics appear normal, as does external examination of her genitalia. She is given an intramuscular injection of progesterone, and 5 days later she has her first period. What is the most likely mechanism responsible for the delay in menses?
In a 40-day menstrual cycle, at which day does ovulation typically occur?
A 23-year-old woman presents for evaluation of a 7-month history of amenorrhea. Examination discloses bilateral galactorrhea and normal breast and pelvic examinations. Pregnancy test is negative. Which of the following classes of medication is a possible cause of her condition?
In Swyer syndrome, what is typically found?
A 20-year-old girl presents with a history of rapidly developing hirsutism and amenorrhea. Which of the following blood tests would be most appropriate to establish the diagnosis?
All are true about hormonal levels in Polycystic Ovarian Disease except?
Practice by Chapter
Hypothalamic-Pituitary-Ovarian Axis
Practice Questions
Disorders of Puberty
Practice Questions
Hirsutism and Virilization
Practice Questions
Primary Ovarian Insufficiency
Practice Questions
Hyperprolactinemia
Practice Questions
Hyperandrogenism
Practice Questions
Metabolic Dysfunction in PCOS
Practice Questions
Neuroendocrine Disorders and Reproduction
Practice Questions
Hormonal Evaluation and Testing
Practice Questions
Ovulation Induction
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app