
Reproductive Endocrinology — MCQs

On this page
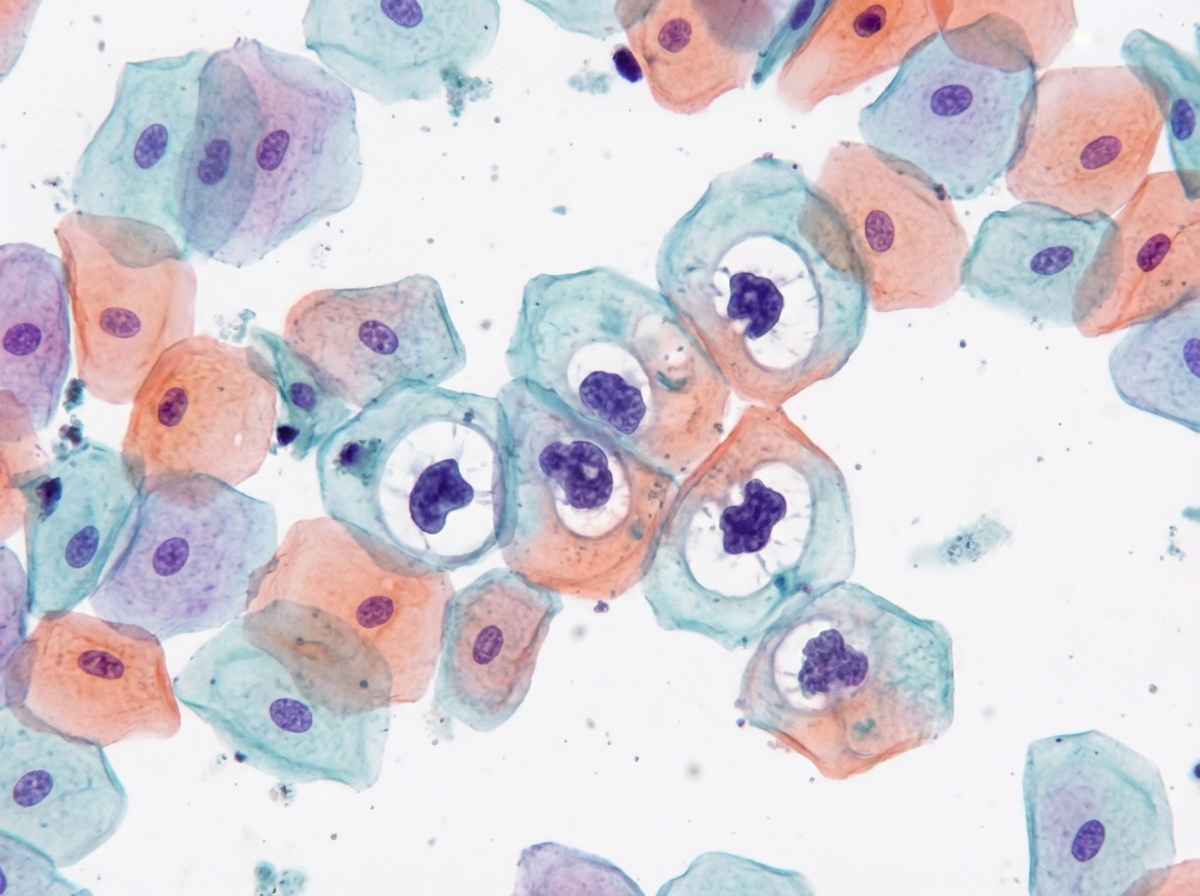
A woman in the late menstrual phase presents with an ovarian mass. Her Pap smear shows predominantly superficial cells stained orange (see image). What is the most likely ovarian tumor?
Which of the following are correct regarding androgen insensitivity syndrome? 1. Inherited as X-linked recessive disorder 2. Karyotype is 46 XXY 3. It is also called testicular feminization 4. Confirmation of diagnosis by gonadal biopsy Select the answer using the code given below.
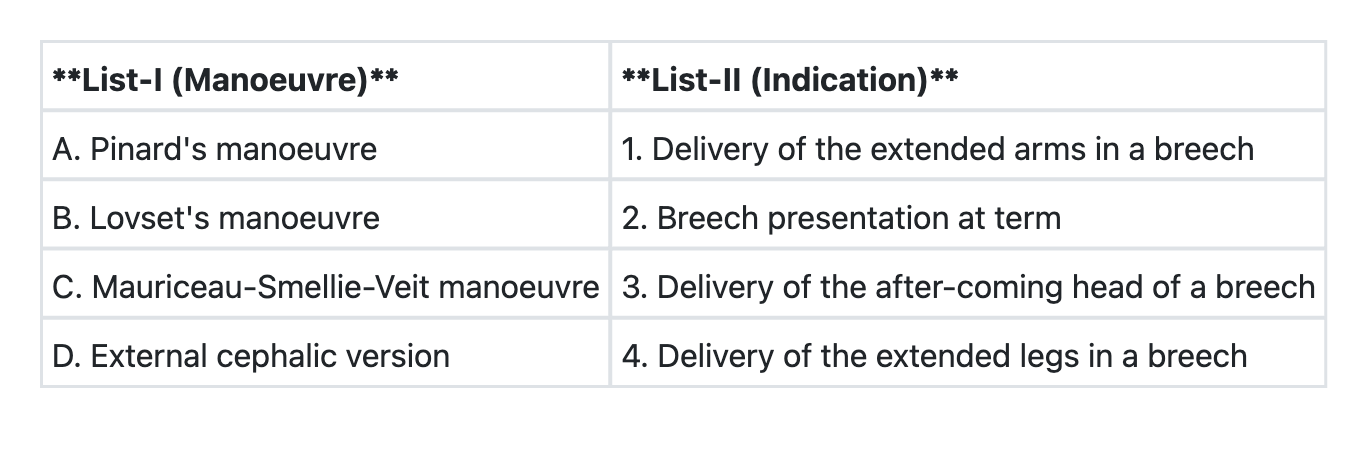
Match List-I with List-II and select the correct answer using the code given below the Lists:
The following hormonal changes mark the Polycystic Ovarian Disease except
If a patient of polycystic ovary syndrome on metformin conceives, how soon should the metformin be stopped?
A 16 year old girl presents with primary amenorrhea with absent vagina, cervix and uterus in the presence of normal secondary sexual characteristics. Ovaries are present on USG. The most probable diagnosis is:
A seven year old girl with precocious puberty is found to be having a 10 cm ovarian cyst on USG. The most likely etiology is
For a primary amenorrhea individual having an XY karyotype, normal infantile female external and internal genitalia, fibrous bands in place of gonads, and lack of development of secondary sexual characters, what is the most probable diagnosis?
Abundant cornified cells in vaginal exfoliative cytology indicate:
Diagnostic criteria for PCOS are: 1. Oligo/amenorrhea 2. Hyperandrogenism 3. Polycystic ovaries on ultrasound Which of the above are correct?
Practice by Chapter
Hypothalamic-Pituitary-Ovarian Axis
Practice Questions
Disorders of Puberty
Practice Questions
Hirsutism and Virilization
Practice Questions
Primary Ovarian Insufficiency
Practice Questions
Hyperprolactinemia
Practice Questions
Hyperandrogenism
Practice Questions
Metabolic Dysfunction in PCOS
Practice Questions
Neuroendocrine Disorders and Reproduction
Practice Questions
Hormonal Evaluation and Testing
Practice Questions
Ovulation Induction
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app