
Reproductive Endocrinology — MCQs

On this page
All of the following are true regarding the use of GnRH analogues in the treatment of endometriosis, EXCEPT?
A 30-year-old female presents with complaints of lethargy, anorexia, weight loss, and secondary amenorrhea. She has a history of postpartum hemorrhage and failed lactation. Which of the following is the most probable diagnosis?
The Fern test is indicative of which physiological change?
A 17-year-old girl presents with primary amenorrhea. On examination, there is absent breast development, but the vagina is normal. Ultrasound reveals a hypoplastic uterus, and bilateral ovaries are not visualized. What is the most likely diagnosis?
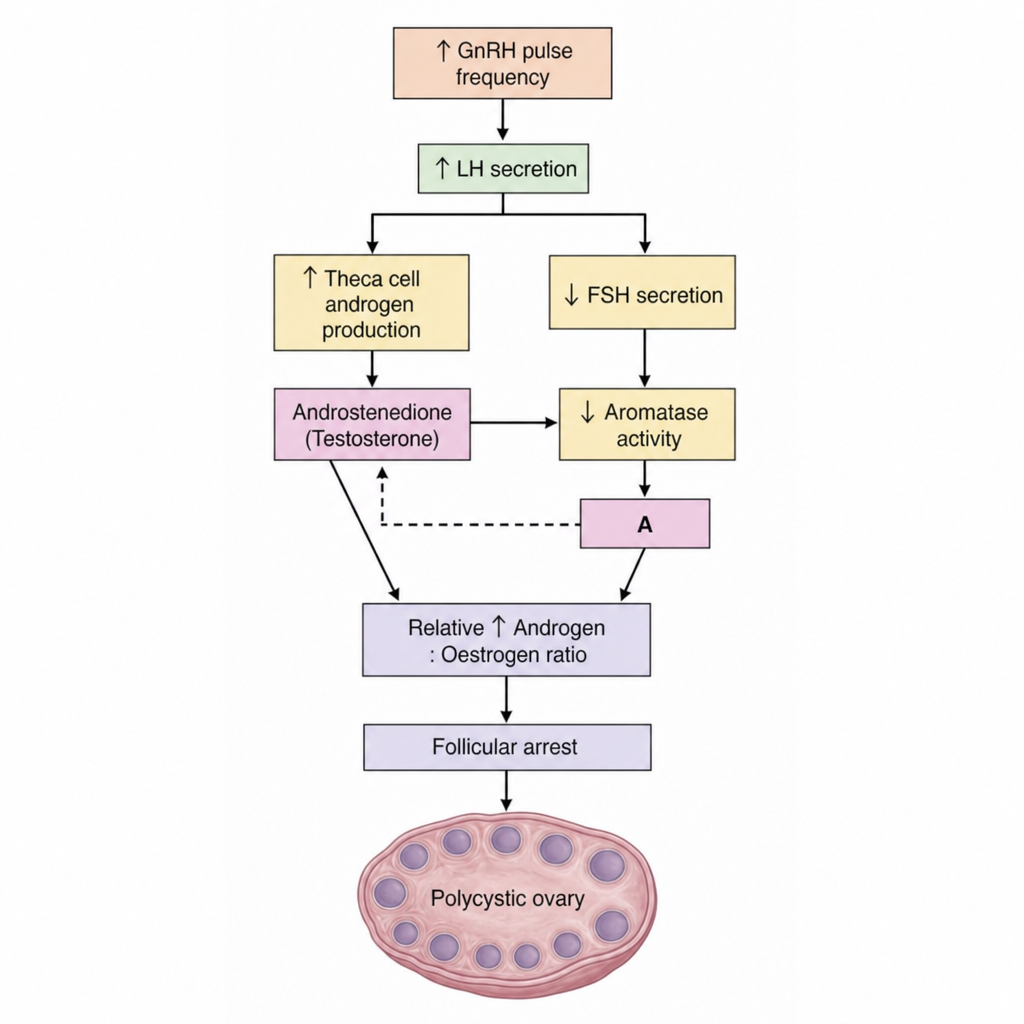
In the given flowchart regarding the pathophysiology of polycystic ovarian syndrome, what does 'A' represent?
What is the primary drug used in the treatment of hirsutism in Polycystic Ovarian Disease (PCOD)?
What is the most common cause of abortion in the first trimester?
A female patient presents with primary amenorrhea. She has a negative progesterone challenge test but a positive response to combined estrogen and progesterone administration. What is the most likely diagnosis?
A patient diagnosed with hypogonadism has normal FSH and estradiol levels. According to the WHO classification of disorders of ovulation, to which type does this patient belong?
All of the following are raised in PCOS except?
Practice by Chapter
Hypothalamic-Pituitary-Ovarian Axis
Practice Questions
Disorders of Puberty
Practice Questions
Hirsutism and Virilization
Practice Questions
Primary Ovarian Insufficiency
Practice Questions
Hyperprolactinemia
Practice Questions
Hyperandrogenism
Practice Questions
Metabolic Dysfunction in PCOS
Practice Questions
Neuroendocrine Disorders and Reproduction
Practice Questions
Hormonal Evaluation and Testing
Practice Questions
Ovulation Induction
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app