
Reproductive Endocrinology — MCQs

On this page
A 12-year-old girl presents with primary amenorrhea. She has been raised as a girl, has not developed breast tissue, and ultrasound reveals absence of the uterus. Karyotyping shows a 46 XY chromosomal pattern. What is the most likely diagnosis?
A 12-year-old female presents with Tanner stage II breast development and white, odorless vaginal discharge. This discharge is most likely due to the action of which hormone?
A 25-year-old female presents with irregular menstrual cycles, acne, and excessive hair growth. An ultrasound reveals multiple ovarian cysts. What is the most likely diagnosis?
A 27-year-old woman presents with irregular periods, acne & excessive hair growth. What is the first line management?
A female presents with hirsutism, delayed periods, obesity. USG findings are given below. What is the likely diagnosis?
A 36-year-old woman presents with secondary amenorrhea for the past 8 months. Laboratory investigations reveal FSH of 36 IU/L and AMH of 0.05 ng/mL. What is the most likely diagnosis?
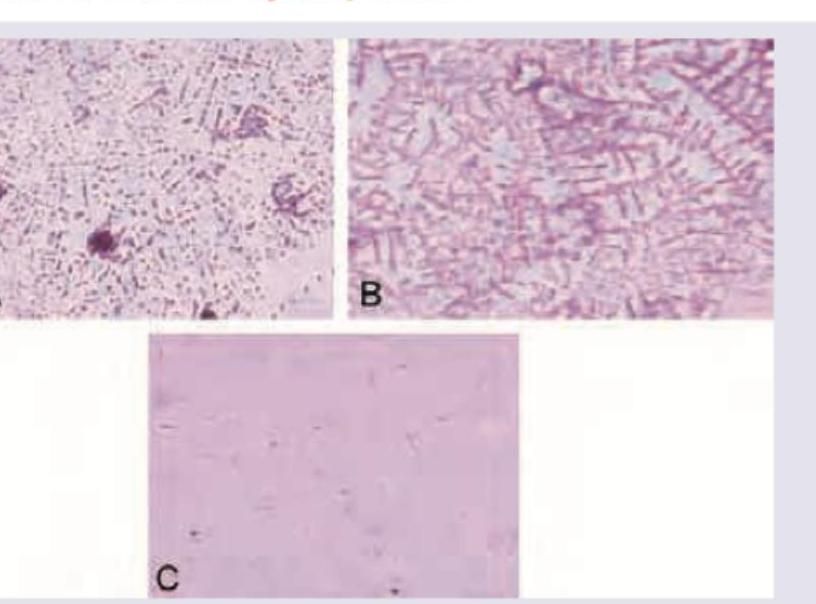
Which of the following cervical mucus smear represents the mid-cycle period?
Which of the following are correct regarding androgen insensitivity syndrome? 1. Inherited as X-linked recessive disorder 2. Karyotype is 46 XXY 3. It is also called testicular feminization 4. Confirmation of diagnosis by gonadal biopsy Select the answer using the code given below.
Which of the following are useful investigations for diagnosis of unresponsive endometrium as a cause of primary amenorrhoea? 1. Karyotype 2. Progesterone challenge test 3. Hormonal studies 4. Hysterosalpingography Select the correct answer using the code given below.
Polycystic ovarian syndrome is associated with the following except
Practice by Chapter
Hypothalamic-Pituitary-Ovarian Axis
Practice Questions
Disorders of Puberty
Practice Questions
Hirsutism and Virilization
Practice Questions
Primary Ovarian Insufficiency
Practice Questions
Hyperprolactinemia
Practice Questions
Hyperandrogenism
Practice Questions
Metabolic Dysfunction in PCOS
Practice Questions
Neuroendocrine Disorders and Reproduction
Practice Questions
Hormonal Evaluation and Testing
Practice Questions
Ovulation Induction
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app