
Follow-up and Future Pregnancy Planning — MCQs

Use of folic acid to prevent congenital malformations should be best initiated:
Most accurate method to confirm viable intrauterine pregnancy at 6 weeks' gestation is
A pregnant lady delivers a healthy baby via normal delivery. What is the earliest time at which an intrauterine contraceptive device (IUCD) can be inserted?
Which of the following is an absolute indication for elective repeat caesarean section in a patient with previous caesarean delivery?
A woman comes after 96 hours post coitus. Best contraceptive of choice is?
A woman dies from a heart disease six days after delivery. This would come under the category of :
The causes for subinvolution of uterus are the following except:
As per the definition of the World Health Organization, 'late maternal death' is defined as the death of a woman from direct or indirect obstetric causes, after more than X days but less than one year after termination of pregnancy. Which one among the following is the correct value of X?
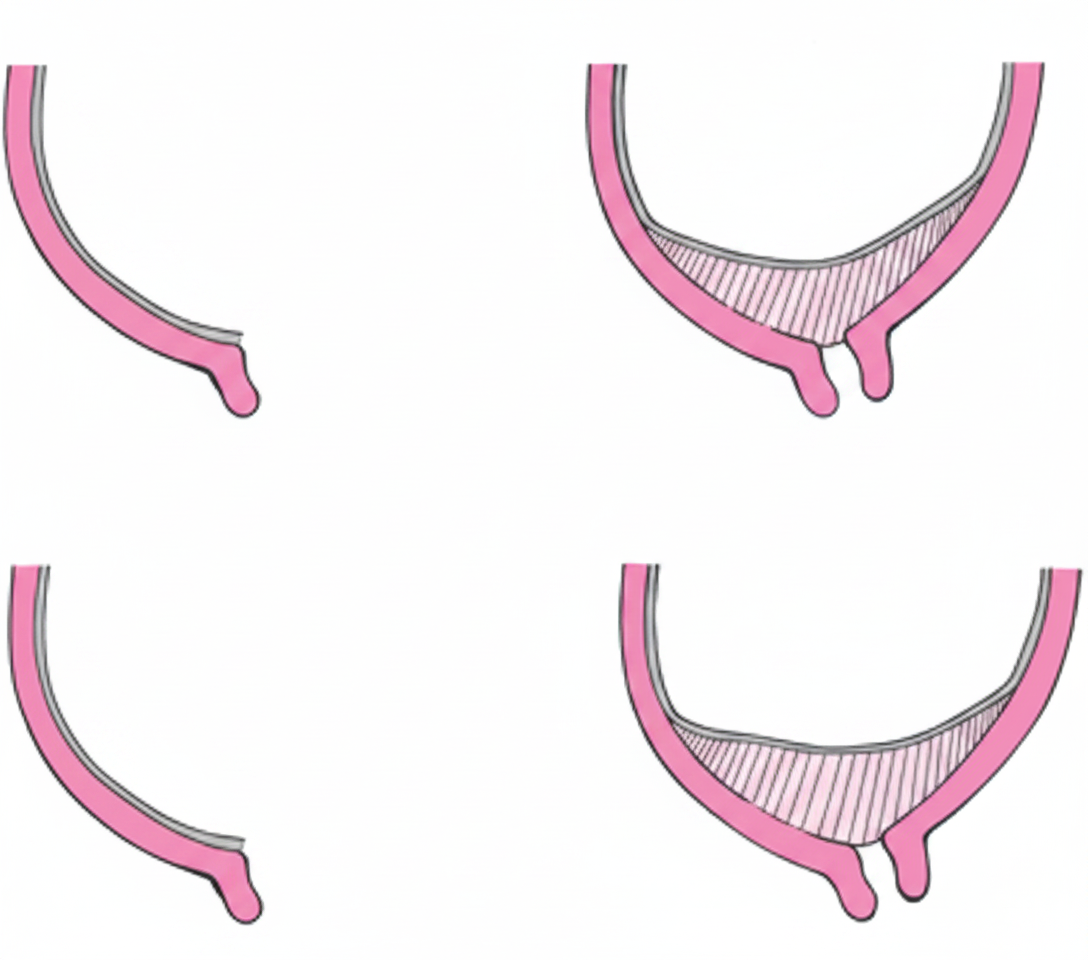
What is the type of placenta previa shown below?
Consider the following regarding the use of Magnesium Sulphate: 1. Used as tocolytic 2. As neuroprotective agent 3. Used in management of postpartum eclampsia Which of the statements given above are correct?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app