
Operative Obstetrics — MCQs

On this page
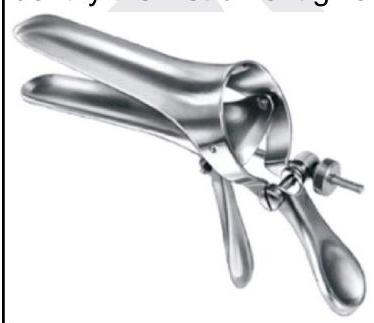
Identify the instrument shown in the image below:

The flexion point in ventouse (vacuum) delivery is located at:
Identify the instrument given below.
Which of the following instruments are used in the caesarean section? 1. Bard-Parker blade 2. Doyen's retractor 3. Cusco's speculum 4. Allis forceps 5. Shirodkar's uterine clamp 6. Green Armytage forceps
A lady with 36-week pregnancy with previous C-section comes with low BP, tachycardia, and on USG fluid present in peritoneum. What is the diagnosis and next management?
Which of these types of fibroid may be removed at the time of a cesarean section?
Which of the following is consistent with a decision to perform a cerclage?
Contraindications to ventouse delivery include all of the following except :
In modern era, the only indication for Internal Podalic Version is:
Shirodkar cerclage may be associated with all complications except:
Practice by Chapter
Cesarean Section Techniques
Practice Questions
Vaginal Birth After Cesarean
Practice Questions
Instrumental Deliveries
Practice Questions
Breech Delivery
Practice Questions
Episiotomy and Repair
Practice Questions
Management of Multiple Gestation
Practice Questions
Cervical Cerclage
Practice Questions
Obstetric Hysterectomy
Practice Questions
Surgery During Pregnancy
Practice Questions
Surgical Complications in Obstetrics
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app