
Operative Obstetrics — MCQs

On this page
The image shows:
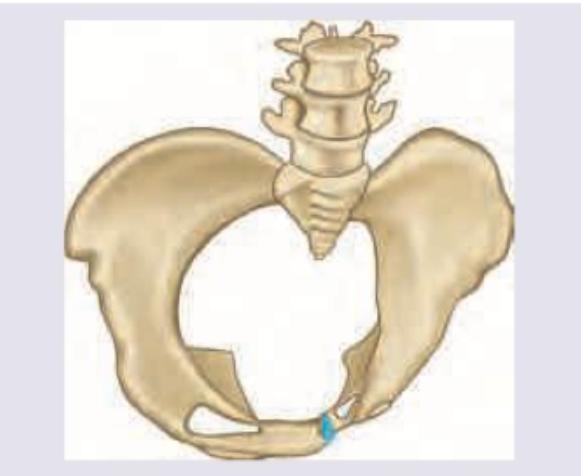
Identify the manoeuvre shown:

Which of the following are contraindications to External Cephalic Version (ECV) in breech? I. Pregnancy less than 36 weeks II. Multiple pregnancy III. Previous cesarean delivery IV. Rhesus isoimmunization Select the correct answer using the code given below :
Which of the following statements are correct regarding audit in Obstetrics and Gynaecology? I. It can replace the out of date clinical practices with better ones. II. It is an efficient educational tool. III. It should be based on scientific evidences with facts and figures. IV. It is not labour-intensive. Select the answer using the code given below :
Which one of the following is an indication for knife conisation? 1. Treatment of Nabothian follicle 2. Diagnosis and directed biopsy of cervix when punch biopsy is inadequate 3. Unsatisfactory colposcopy (transformation zone not fully visible) 4. Negative endocervical curettage Select the correct answer using the code given below:
Which one of the following is a prerequisite for Endometrial Ablation ?
Which of the following are essential steps of Fothergill's operation? 1. Laparoscopic or vaginal ligation 2. Amputation of cervix 3. Plication of Mackenrodt's ligaments in front of cervix 4. Anterior colporrhaphy Select the correct answer using the code given below.
Which of the following is a common pathology that increases the risk of uterine injury during abdominal hysterectomy?
Spiegelberg's criteria for diagnosis of ovarian pregnancy include the following except
A multiparous woman presenting with postpartum haemorrhage due to placenta increta is best managed by
Practice by Chapter
Cesarean Section Techniques
Practice Questions
Vaginal Birth After Cesarean
Practice Questions
Instrumental Deliveries
Practice Questions
Breech Delivery
Practice Questions
Episiotomy and Repair
Practice Questions
Management of Multiple Gestation
Practice Questions
Cervical Cerclage
Practice Questions
Obstetric Hysterectomy
Practice Questions
Surgery During Pregnancy
Practice Questions
Surgical Complications in Obstetrics
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app