
Operative Obstetrics — MCQs

On this page
B-Lynch suture for atonic postpartum haemorrhage:
In the process of MTP (Medical Termination of Pregnancy) done by suction and evacuation, it was realized that perforation of uterus occurred with cannula. The next step should be:
Which of the following are the pre-requisites of outlet forceps delivery? 1. Bladder should be empty 2. Membranes should be intact 3. Cervix should be fully dilated 4. Fetal skull has reached level of pelvic floor
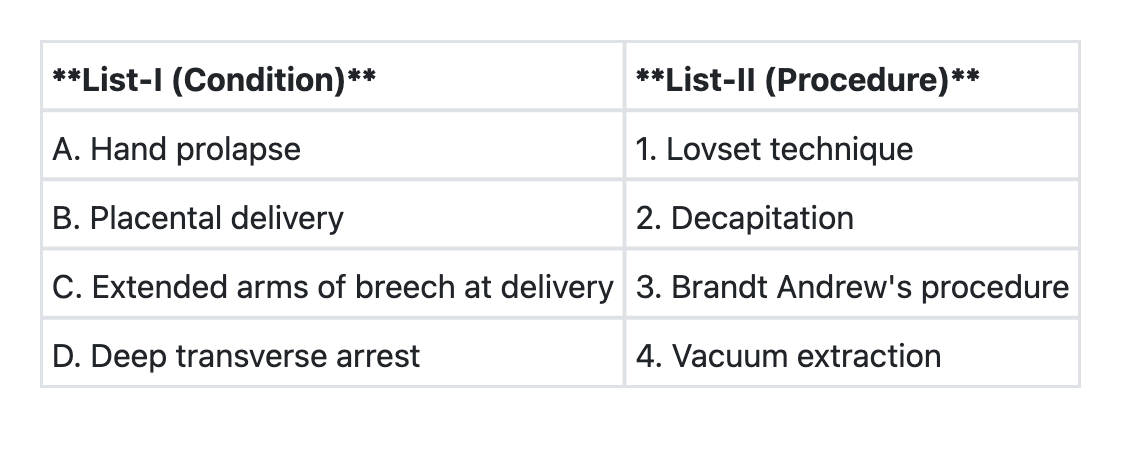
Match List-I with List-II and select the correct answer using the code given below the Lists:
Which one of the following is not a suitable condition for outlet forceps application?
Identify the maneuver shown in panel A of the image:
Identify the instrument shown in the image below: 

Identify the instrument shown in the image below:

The flexion point in ventouse (vacuum) delivery is located at:
Which of the following instruments are used in the caesarean section? 1. Bard-Parker blade 2. Doyen's retractor 3. Cusco's speculum 4. Allis forceps 5. Shirodkar's uterine clamp 6. Green Armytage forceps
Practice by Chapter
Cesarean Section Techniques
Practice Questions
Vaginal Birth After Cesarean
Practice Questions
Instrumental Deliveries
Practice Questions
Breech Delivery
Practice Questions
Episiotomy and Repair
Practice Questions
Management of Multiple Gestation
Practice Questions
Cervical Cerclage
Practice Questions
Obstetric Hysterectomy
Practice Questions
Surgery During Pregnancy
Practice Questions
Surgical Complications in Obstetrics
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app