
Operative Obstetrics — MCQs

On this page
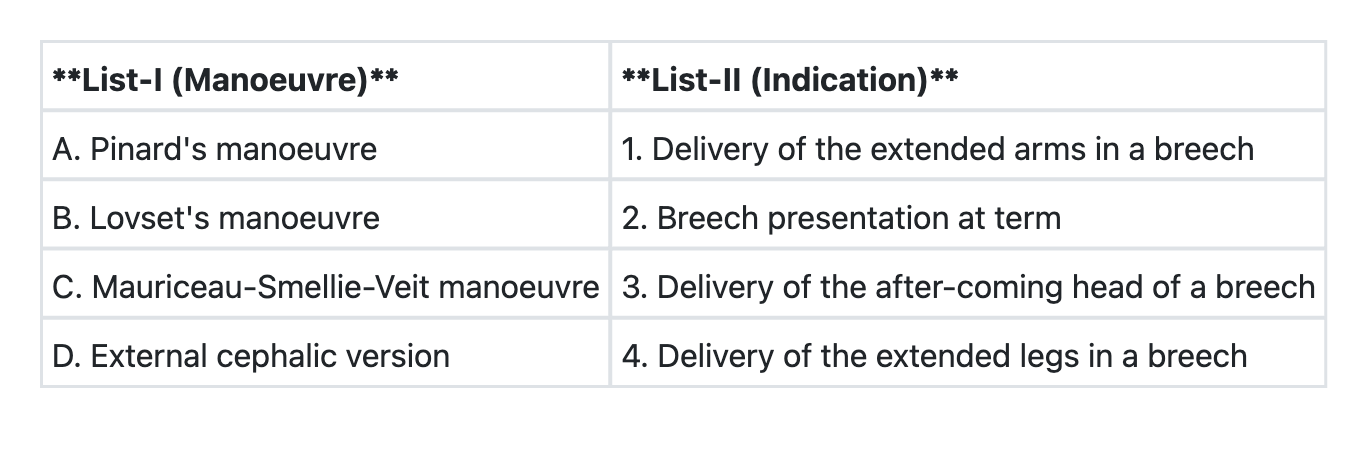
Match List-I with List-II and select the correct answer using the code given below the Lists:
Use of ventose is preferred over forceps in the delivery of :
A multiparous woman presenting with postpartum haemorrhage due to placenta increta is best managed by
A 34-week multiparous gravida comes in labour. On examination, the cervix is fully dilated, the head is at +2 station and the foetal heart rate is 172/min. The appropriate management will be
A second gravida, whose first baby is alive, has been in the second stage of labour for more than one hour. On examination, her cervix is fully dilated. The pelvis is adequate and the station of the vertex is +2. The occiput is in right, occipito-posterior position and the fetal heart rate is 120/min. The most appropriate management will be
A pregnant mother is referred with a prolonged second stage of labour. On examination, the foetal heart sound is 120/min, and the head is at -1 station with severe moulding. What will be the most appropriate management?
The indications of an elective caesarean section include all of the following, except
Regarding the use of a ventouse, which one of the following statements is not correct?
A 20-year-old nulli-term primigravida is brought to the casualty with labour pains for last 24 hours and a hand prolapse. On examination, she has pulse 96/min, BP 120/80 mm Hg, and mild pallor. The abdominal examination reveals the uterine height at 32 weeks, the foetus in transverse lie and absent foetal heart sounds. On vaginal examination, the left arm of the foetus is prolapsed and the foetal ribs are palpable. The pelvis is adequate. What would be the best management option?
Which of the following is the most appropriate management in a ruptured tubal pregnancy?
Practice by Chapter
Cesarean Section Techniques
Practice Questions
Vaginal Birth After Cesarean
Practice Questions
Instrumental Deliveries
Practice Questions
Breech Delivery
Practice Questions
Episiotomy and Repair
Practice Questions
Management of Multiple Gestation
Practice Questions
Cervical Cerclage
Practice Questions
Obstetric Hysterectomy
Practice Questions
Surgery During Pregnancy
Practice Questions
Surgical Complications in Obstetrics
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app