
Operative Obstetrics — MCQs

On this page
In the repair of a mediolateral episiotomy, what is the correct order of tissue closure?
Identify the instrument shown:
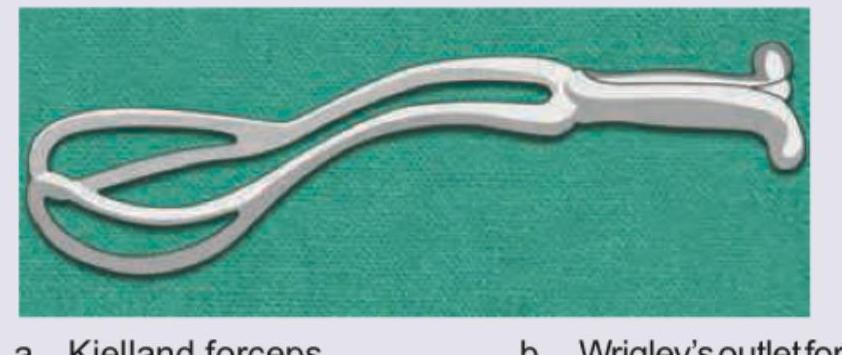
Identify the instrument shown:

All are correct regarding the device shown here except:

The following manoeuvre is called:

The following manoeuvre is called:
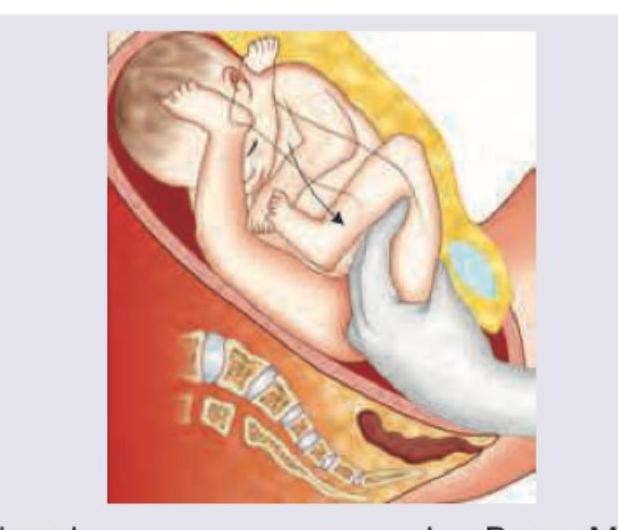
Identify the manoeuvre shown:

Identify the instrument used: (AIIMS Nov 2017)

Which of the following are contraindications to External Cephalic Version (ECV) in breech? I. Pregnancy less than 36 weeks II. Multiple pregnancy III. Previous cesarean delivery IV. Rhesus isoimmunization Select the correct answer using the code given below :
Indications and prerequisites for delivery with the ventouse include which of the following? 1. Delay in the second stage of labour 2. Non-reassuring fetal heart rate 3. Gestation age less than 34 weeks of pregnancy 4. Vertex presentation.
Practice by Chapter
Cesarean Section Techniques
Practice Questions
Vaginal Birth After Cesarean
Practice Questions
Instrumental Deliveries
Practice Questions
Breech Delivery
Practice Questions
Episiotomy and Repair
Practice Questions
Management of Multiple Gestation
Practice Questions
Cervical Cerclage
Practice Questions
Obstetric Hysterectomy
Practice Questions
Surgery During Pregnancy
Practice Questions
Surgical Complications in Obstetrics
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app