
Menstrual Disorders — MCQs

On this page
Causes of AUB are subdivided by the acronym PALM-COEIN. What are the characteristics of PALM causes? I. Structural lesions II. Diagnosed by ultrasound III. Confirmed by histopathology Select the correct answer using the code given below :
Which one of the following is a prerequisite for Endometrial Ablation ?
A 16-year-old girl with primary amenorrhoea presents to the gynaecology OPD for evaluation. She has normal secondary sexual characters. Her karyotype is 46,XX and ultrasound reveals normal ovaries and tubes but absent uterus. What is her clinical diagnosis?
A 25-year-old female comes to the gynaecology OPD for evaluation of secondary amenorrhoea. She gives history of previous dilatation and curettage, and her FSH levels are 8 IU/L. The probable cause of amenorrhoea is
Premenstrual Syndrome (PMS) should fulfil which of the following criteria? 1. It is not related to any organic lesion. 2. It regularly occurs during the luteal phase and each ovulatory menstruation cycle. 3. Symptoms must be severe enough to disturb the lifestyle of women and seeks medical help. 4. Symptoms persist after the period also.
In the PALM-COEIN classification by FIGO for abnormal uterine bleeding, ovulatory dysfunction is the cause in which one of the following conditions?
Which of the following is MOST effective as a first-line management for premenstrual syndrome?
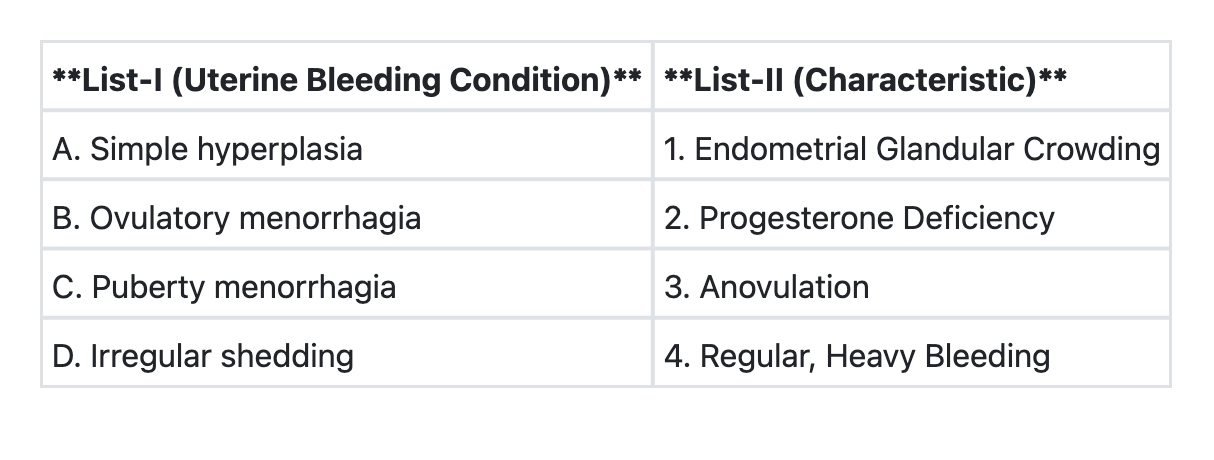
Match List-I with List-II and select the correct answer using the code given below the Lists:
The following drugs are effective in the management of menorrhagia except :
A 15-year old unmarried girl comes with history of dysmenorrhea. Age of menarche is 12 years. Per abdominal and per rectum examination reveal nothing abnormal. You will treat the patient with :
Practice by Chapter
Normal Menstrual Physiology
Practice Questions
Primary Dysmenorrhea
Practice Questions
Secondary Dysmenorrhea
Practice Questions
Premenstrual Syndrome and PMDD
Practice Questions
Primary Amenorrhea
Practice Questions
Secondary Amenorrhea
Practice Questions
Polycystic Ovary Syndrome
Practice Questions
Abnormal Uterine Bleeding: Classification
Practice Questions
Evaluation of Menstrual Disorders
Practice Questions
Management Approaches to Menstrual Disorders
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app