
Abnormal Uterine Bleeding: Classification — MCQs

Most common uterine tumor is:-
35 yr old lady attends gynaec OPD with excessive bleeding since 6 months, not controlled with non hormonal drugs. USG and clinical examination reveals no abnormality. Next step is?
Most useful investigation in a 55-year-old postmenopausal woman with diabetes mellitus and hypertension who has presented with postmenopausal bleeding is:
A postmenopausal diabetic woman presents with bleeding per vaginum. The most likely diagnosis is :
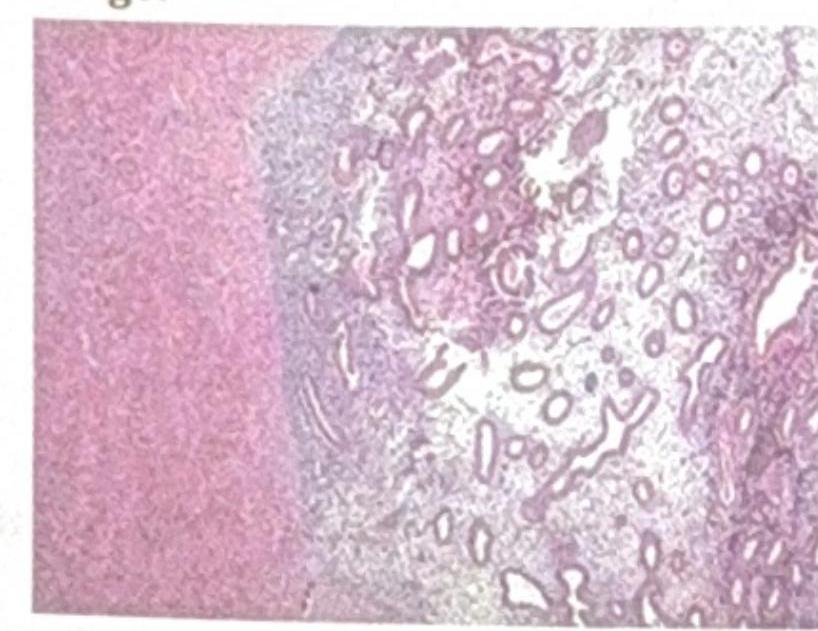
Identify the pathological condition shown in the image:
An 18-year-old unmarried girl comes with complaints of heavy, prolonged bleeding during menses. Which among the following investigations is NOT usually advised?
Dysfunctional uterine bleeding (DUB) is best treated by:
A 32-year-old woman presents with irregular, heavy menstrual bleeding. After thorough evaluation including pelvic ultrasound, hormonal assays, coagulation profile, and endometrial sampling, no structural abnormalities, systemic disorders, or medication-related causes are identified. This clinical scenario is best described as:
A 45 year old woman presents with continuous vaginal bleeding for 15 days. Her bleeding should be controlled by:
A 20-year-old married woman anxious to get pregnant has cyclical cramps and sharp lower abdominal pain which lasts for 3 days starting from the day of her menstrual flow. Her menstrual periods are regular but heavy. On clinical examination, her pelvis is normal. The most probable diagnosis is
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app