
Maternal-Fetal Medicine — MCQs

On this page
During a routine prenatal visit, a 22-week gravid woman is found to be affected with ankle oedema and new onset hypertension. The urine analysis reveals marked proteinuria. Which of the following, if it were to occur, would substantiate the diagnosis of eclampsia?
In a pregnancy complicated by heart disease, which of the following is/are contraindicated? 1. External cephalic version 2. LSCS 3. Corrective surgery of the heart lesion 4. Prophylactic intravenous meth-ergine at the birth of anterior shoulder Select the correct answer from the code given below :
A nulliparous woman presents with acute lower abdominal pain. She has a history of missed periods. The ultrasound examination shows an empty uterus. The cervical movements are very tender. The vital signs are stable. How will you manage her?
Antimicrobial prophylaxis is essential for a woman in labour who has
The perinatal complications of a diabetic pregnancy include : 1. Small for Gestational Age baby 2. Stillbirth 3. Hypoglycaemia 4. Respiratory distress syndrome Select the correct answer from the code given below :
Abortions in the second trimester mainly occur due to
Which one of the following is diagnosed by Spiegelberg criteria?
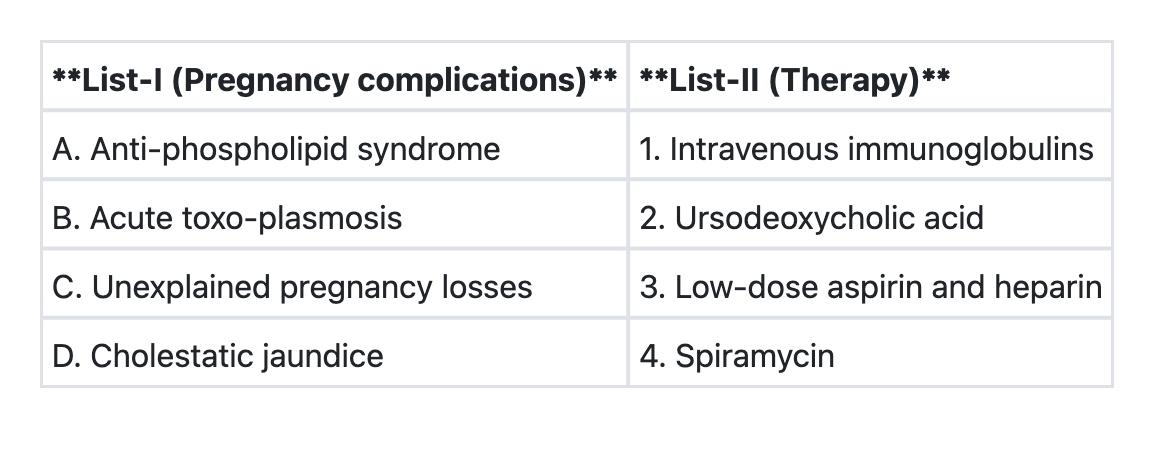
Match List-I with List-II and select the correct answer using the code given below the Lists:
The fetal well-being can be assessed by all of the following, except
With reference to the transmission of HIV from mother to child, which one of the following statements is not correct?
Practice by Chapter
Fetal Assessment Techniques
Practice Questions
Hypertensive Disorders in Pregnancy
Practice Questions
Intrauterine Growth Restriction
Practice Questions
Multiple Gestation
Practice Questions
Rh Isoimmunization and Other Blood Group Incompatibilities
Practice Questions
Intrauterine Fetal Therapy
Practice Questions
Prenatal Diagnosis and Genetic Counseling
Practice Questions
Placental Abnormalities
Practice Questions
Preterm Labor and Delivery
Practice Questions
Management of Medical Disorders in Pregnancy
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app