
Maternal-Fetal Medicine — MCQs

On this page
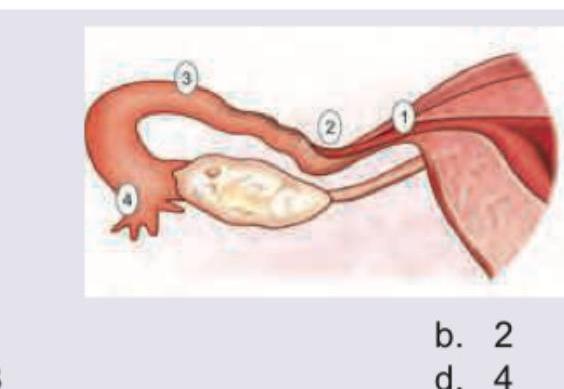
A 25-year-old lady had tubal rupture due to ectopic pregnancy at 6 weeks. Which of the following sites is most likely to rupture earliest in an ectopic pregnancy?
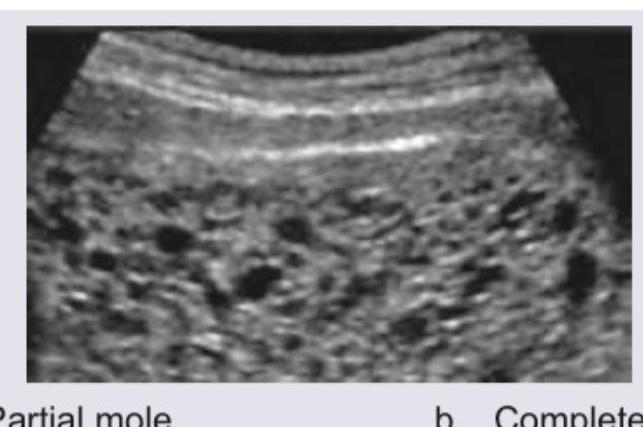
A 25-year-old presents with amenorrhea of 8 weeks. Ultrasound shows a thickened, heterogeneous placenta with multiple cystic spaces and a small, abnormal gestational sac. What does the USG show?
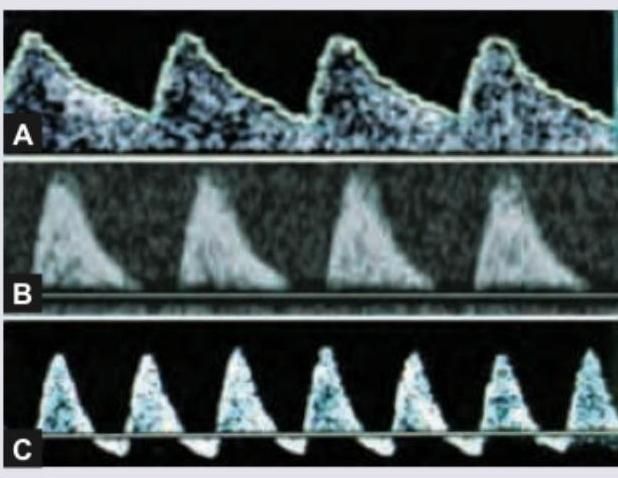
Between the three studies of fetal umbilical artery velocimetry by Doppler USG, which one will have the highest chances of fetal compromise?
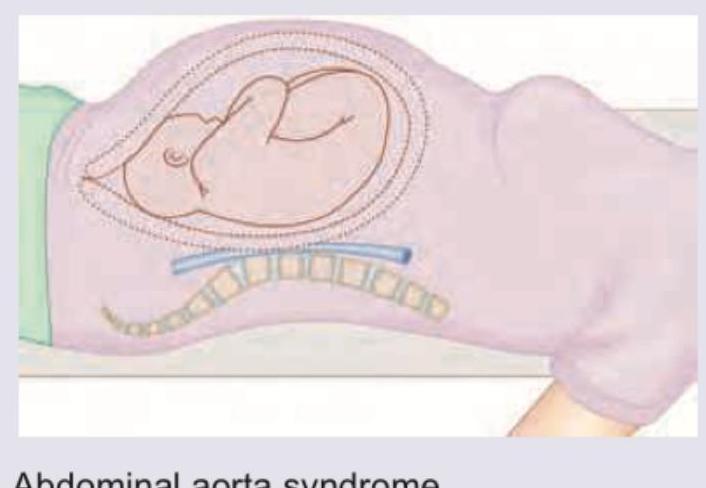
A pregnant lady was admitted with diagnosis of PIH for monitoring and bed rest. When lying in supine position, which of the following complications is depicted in the image below?
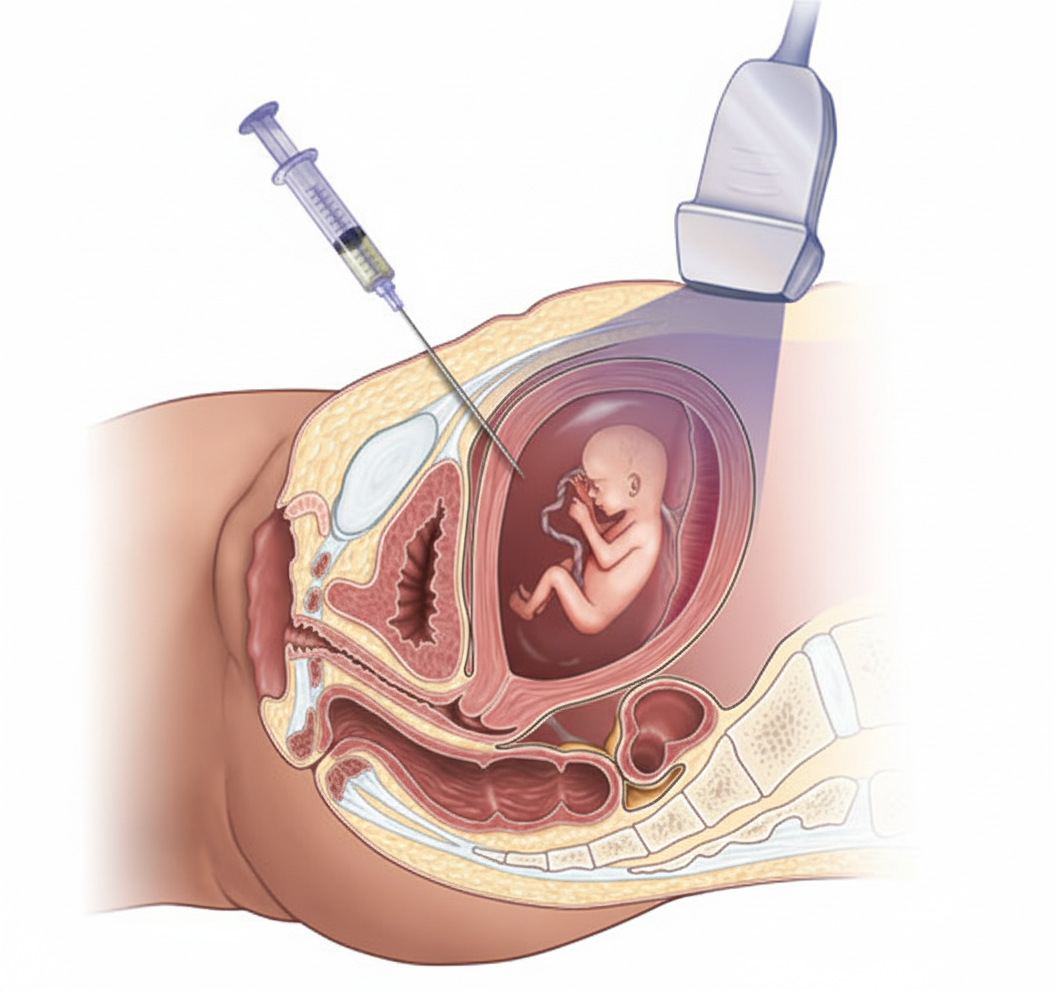
What procedure is being demonstrated in the image?
Increased nuchal translucency is a feature of:
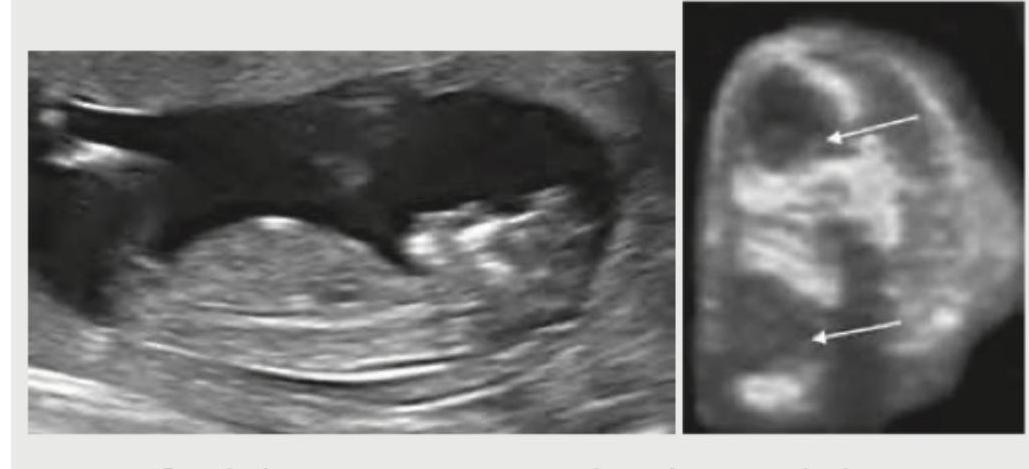
A 21-year-old G2P1 presents to OPD at 20 weeks of gestation for a second opinion since her family physician had told her that the foetus had some problem. Her obstetric USG is given below. What is the diagnosis? (AIIMS May 2016)
Which of the following maternal complications can be seen in hyperemesis gravidarum? I. Wernicke's encephalopathy II. Hepatic failure III. Hypoprothrombinemia IV. Convulsions Select the correct answer using the code given below :
Twin pregnancy should have ultrasound at 10-13 weeks to confirm which of the following? I. Number of foetus II. Viability of foetus III. Chorionicity of twins IV. Malformation in either foetus Select the correct answer using the code given below :
Which of the following is the primary surveillance tool in the growth-restricted fetus?
Practice by Chapter
Fetal Assessment Techniques
Practice Questions
Hypertensive Disorders in Pregnancy
Practice Questions
Intrauterine Growth Restriction
Practice Questions
Multiple Gestation
Practice Questions
Rh Isoimmunization and Other Blood Group Incompatibilities
Practice Questions
Intrauterine Fetal Therapy
Practice Questions
Prenatal Diagnosis and Genetic Counseling
Practice Questions
Placental Abnormalities
Practice Questions
Preterm Labor and Delivery
Practice Questions
Management of Medical Disorders in Pregnancy
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app