
Maternal-Fetal Medicine — MCQs

On this page
The following diagram shows:
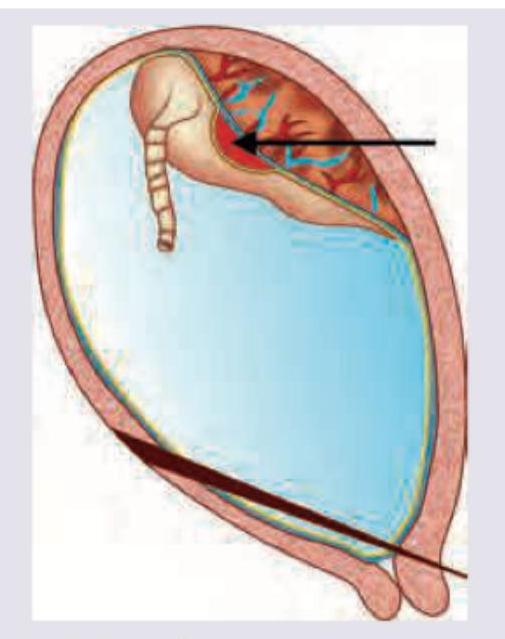
The optical density of amniotic fluid at 450 nm peak was plotted on Liley's chart and falls in zone marked as C. Which of the following statements is correct?
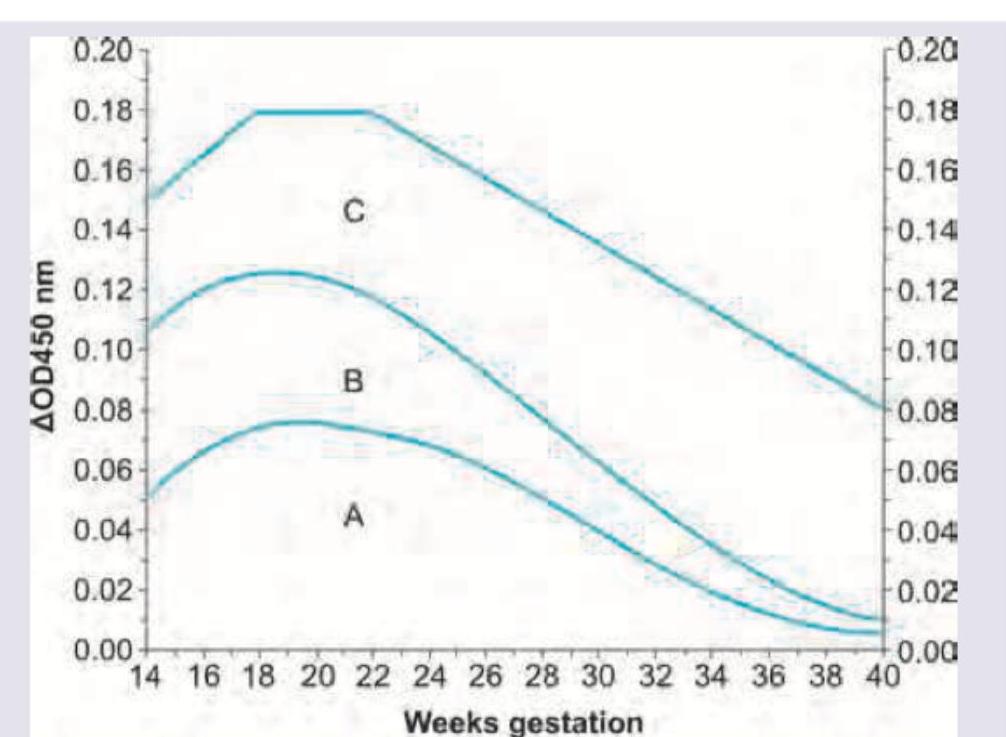
The following curve is used in evaluation of:
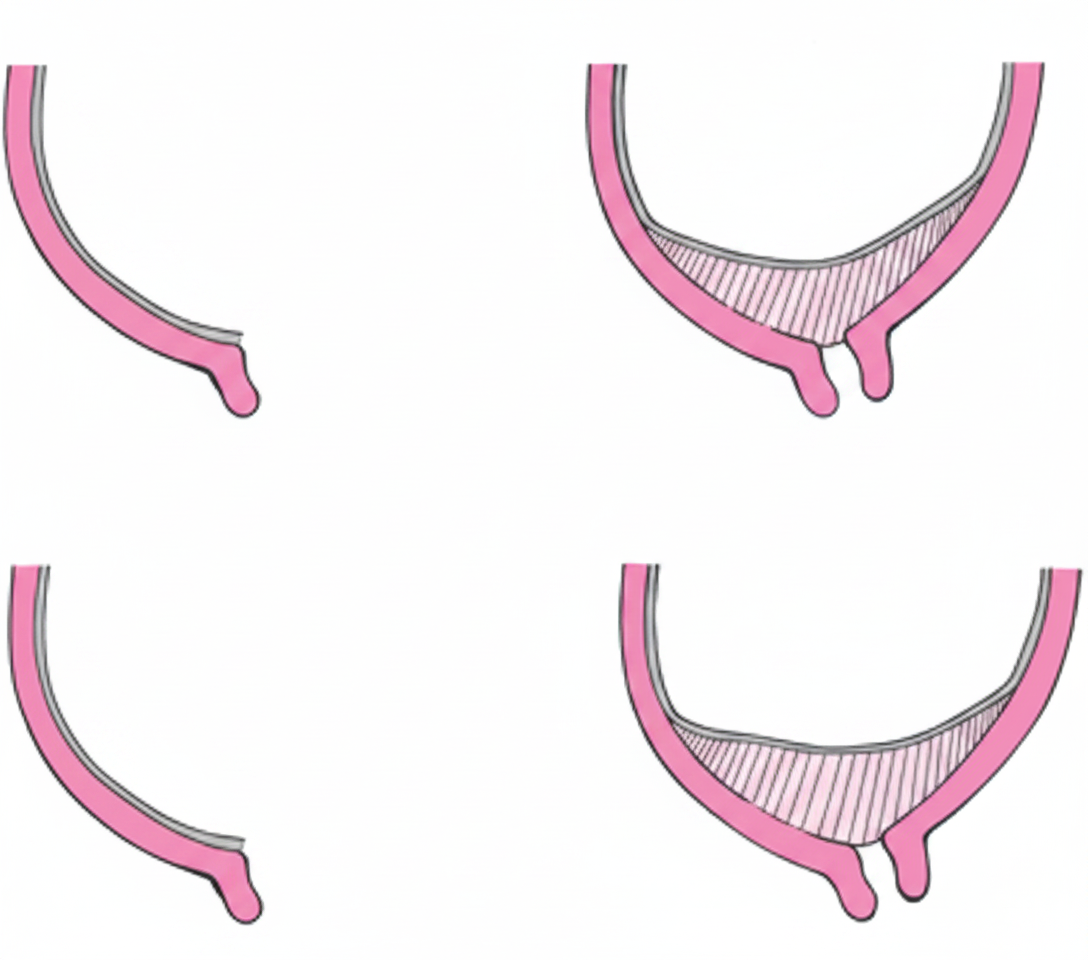
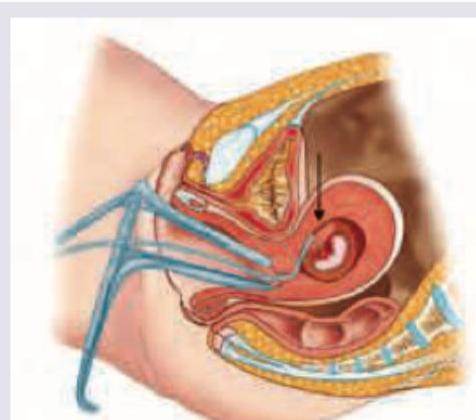
What is the type of placenta previa shown below?
Vasa previa is a complication of which of the following types of placenta?
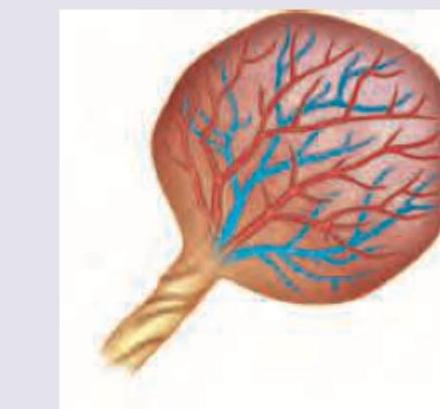
Which of the following is correct about the placenta shown below? (Recent NEET Pattern 2016-17)

What is the type of placenta shown below?
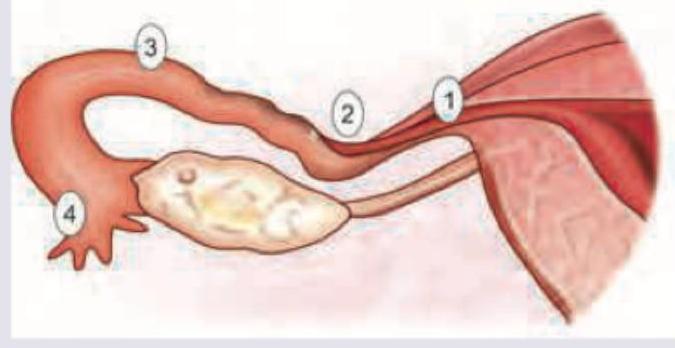
The image shows:
The least common site of ectopic pregnancy is:
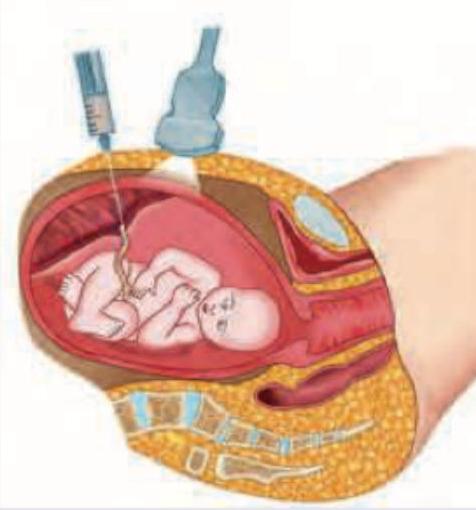
The image shows an ultrasound-guided procedure with a needle inserted into a fetal structure. What is this procedure called?
Practice by Chapter
Fetal Assessment Techniques
Practice Questions
Hypertensive Disorders in Pregnancy
Practice Questions
Intrauterine Growth Restriction
Practice Questions
Multiple Gestation
Practice Questions
Rh Isoimmunization and Other Blood Group Incompatibilities
Practice Questions
Intrauterine Fetal Therapy
Practice Questions
Prenatal Diagnosis and Genetic Counseling
Practice Questions
Placental Abnormalities
Practice Questions
Preterm Labor and Delivery
Practice Questions
Management of Medical Disorders in Pregnancy
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app