
Maternal-Fetal Medicine — MCQs

On this page
A primigravida woman at 26 weeks gestation, presented with a BP of 150/90 mm Hg. Which test should be done next?
A 32-year-old woman at 32 weeks gestation presents with sudden-onset severe abdominal pain and vaginal bleeding. She has a history of cocaine use. On examination, the uterus is tender, firm, and woody hard. Fetal heart sounds are absent. Blood pressure is 90/60 mmHg, pulse 120/min. What is the most likely diagnosis?
Which of the following does not cause fetal bradycardia?
Use of magnesium sulfate (MgSO4) in pre-eclampsia has all of the following effects except:
A 36-week pregnant woman is diagnosed with preeclampsia and started on magnesium sulfate therapy. According to the Pritchard regimen, what is the total loading dose of magnesium sulfate administered initially?
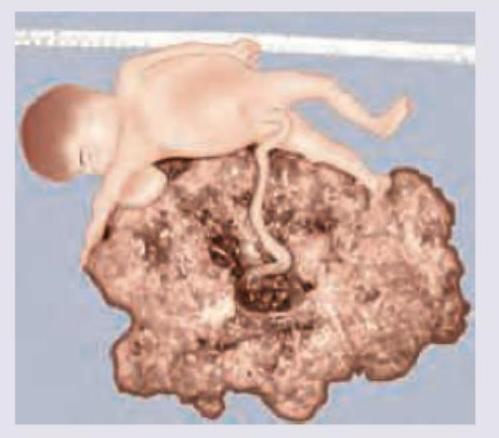
Identify the type of conjoined twins shown below.

A patient presents with vaginal bleeding in the first trimester. Histopathological examination of the products of conception reveals the findings shown in the image below. What is the most likely diagnosis?
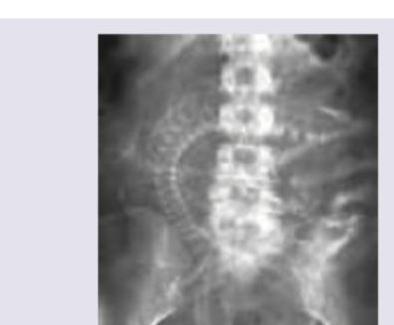
The image shows the X-ray abdomen of a 30-yearold SLE patient, with ultrasound-confirmed intrauterine fetal demise retained for more than 4 weeks, who cannot feel her baby moving for the past 7 days, and whose coagulation workup shows low fibrinogen with elevated D-dimer consistent with consumption coagulopathy. All are correct about the condition shown except:
What is incorrect about the neonate shown:

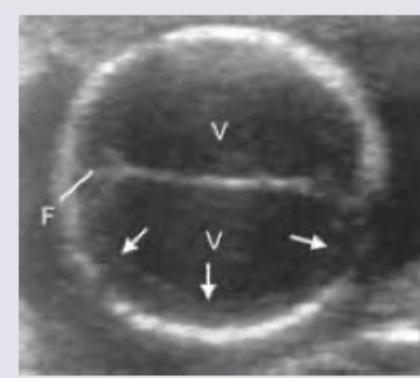
A gynecologist noted that fetal head is difficult to push down into the pelvis at 36 weeks of gestation. Antenatal USG done shows presence of:
Practice by Chapter
Fetal Assessment Techniques
Practice Questions
Hypertensive Disorders in Pregnancy
Practice Questions
Intrauterine Growth Restriction
Practice Questions
Multiple Gestation
Practice Questions
Rh Isoimmunization and Other Blood Group Incompatibilities
Practice Questions
Intrauterine Fetal Therapy
Practice Questions
Prenatal Diagnosis and Genetic Counseling
Practice Questions
Placental Abnormalities
Practice Questions
Preterm Labor and Delivery
Practice Questions
Management of Medical Disorders in Pregnancy
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app