
Maternal-Fetal Medicine — MCQs

On this page
A patient with a known marginal placenta presents for follow-up. On ultrasound, a 4 x 4 cm placental mass is noted invading into the urinary bladder. What is the most likely diagnosis?
Fetal anaemia is primarily determined by Doppler assessment of which artery?
A 28-year-old pregnant woman at 33 weeks gestation presents for a routine prenatal visit. She reports decreased fetal movements over the past two days. She has a history of gestational diabetes, and her pregnancy has been otherwise uneventful. The doctor decides to perform antepartum fetal surveillance. Which of the following is the most appropriate initial test to assess the fetal well-being in this scenario?
A 29-year-old woman presents with abdominal pain, vaginal bleeding, and a history of amenorrhea for 6 weeks. Transvaginal ultrasound does not show an intrauterine gestational sac or features suggestive of ectopic pregnancy. Her serum $\beta$-hCG is 1,200 IU/L, which is below the discriminatory zone. What is the next step in management?
Fetal anaemia is monitored by?
Which of the following drugs is not given for hypertension in pregnancy?
Which findings are most suggestive of tubal pregnancy?
Identify the given image of the placenta previa (using the historical classification).
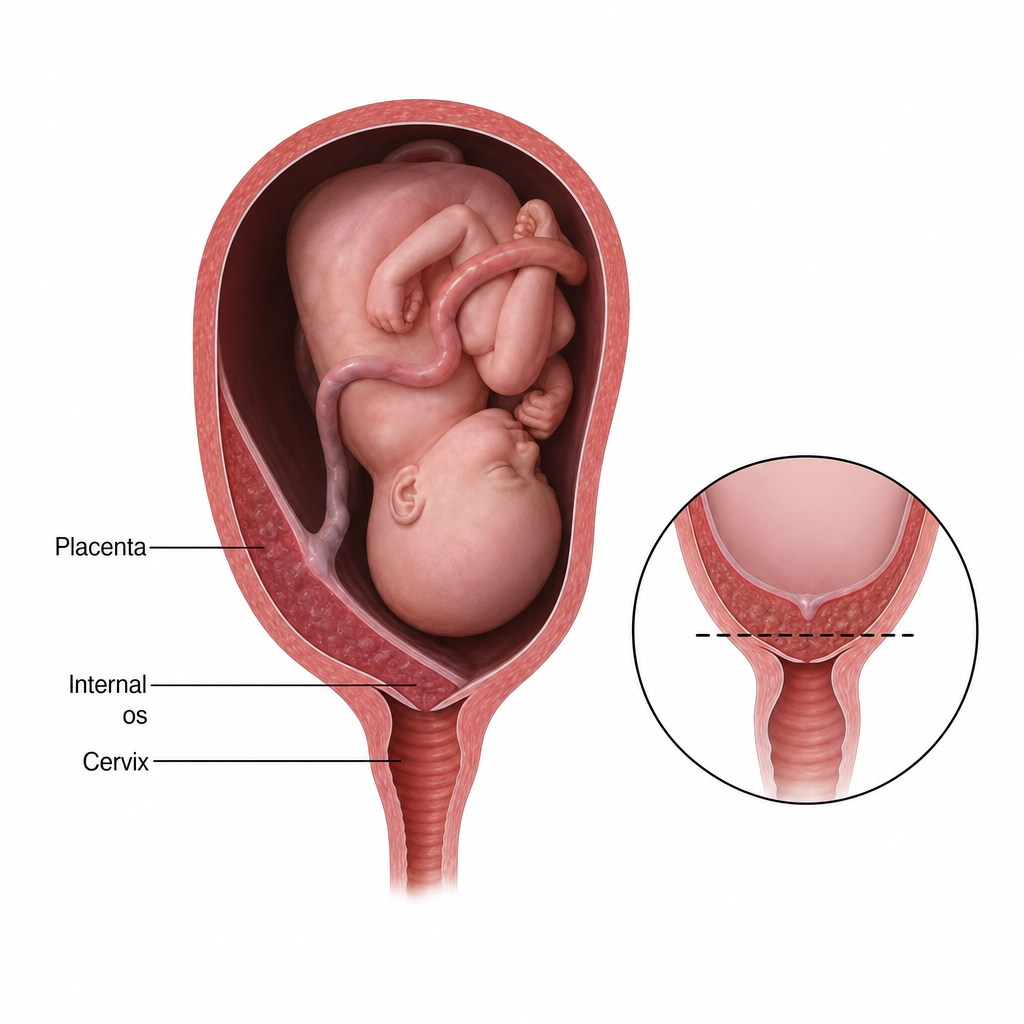
Identify the given image of the placenta previa using the historical (older) classification system. 
Which of the following is the most common location of implantation in ectopic pregnancy? 
Practice by Chapter
Fetal Assessment Techniques
Practice Questions
Hypertensive Disorders in Pregnancy
Practice Questions
Intrauterine Growth Restriction
Practice Questions
Multiple Gestation
Practice Questions
Rh Isoimmunization and Other Blood Group Incompatibilities
Practice Questions
Intrauterine Fetal Therapy
Practice Questions
Prenatal Diagnosis and Genetic Counseling
Practice Questions
Placental Abnormalities
Practice Questions
Preterm Labor and Delivery
Practice Questions
Management of Medical Disorders in Pregnancy
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app