
Maternal-Fetal Medicine — MCQs

On this page
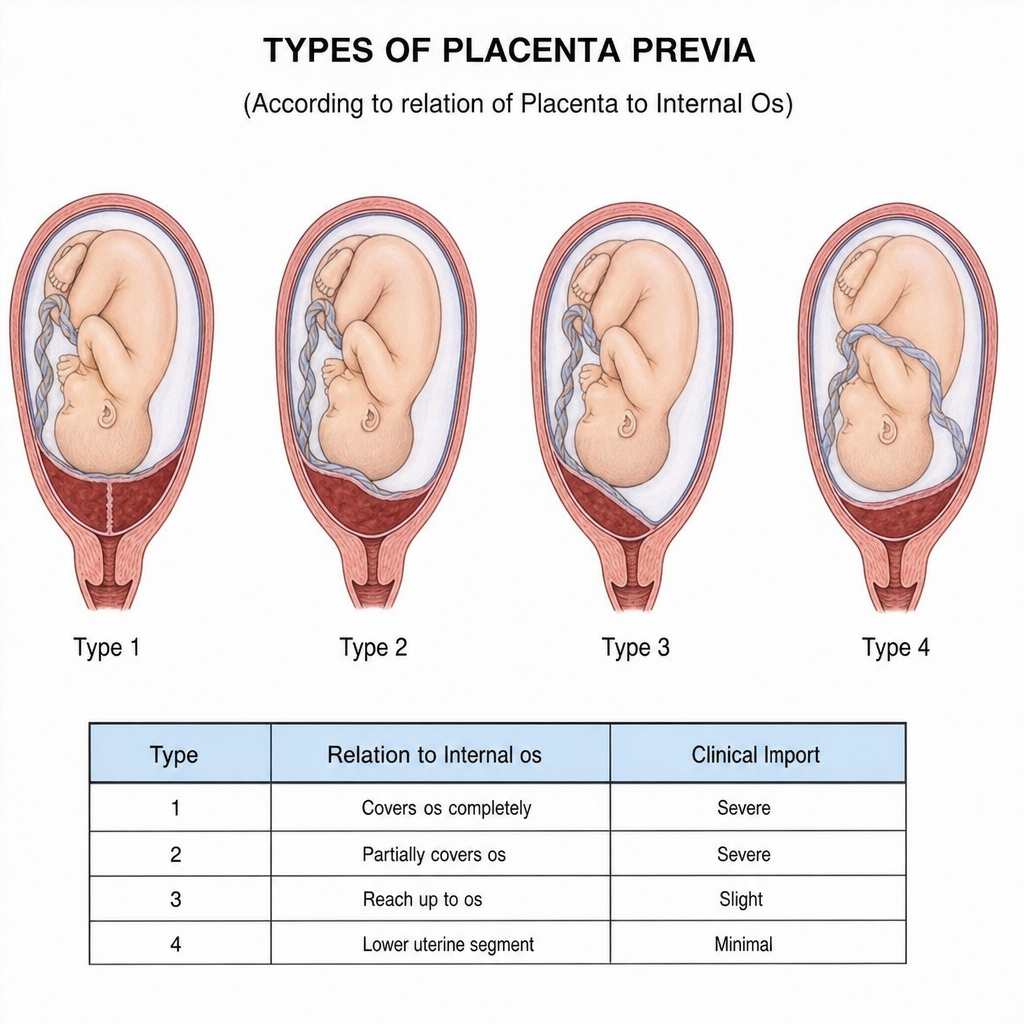
A 30-week gestation patient presents with a history of vaginal bleeding and is admitted for evaluation. Fetal heart rate is 130 bpm with normal variability. Ultrasonography reveals a placenta partially covering the internal cervical os. Currently, there is no active vaginal bleeding. What is the best management for this patient?
All of the following are used in inherited thrombophilia testing in pregnancy, except:
Which type of placenta previa is described?
In accidental hemorrhage, what is the definitive treatment?
MgSO4 is contraindicated in eclampsia during treatment EXCEPT when which of the following occurs?
A Rh negative G4P3+0 patient has an antibody level of 15 IU/ml (IAT 1:32) at 27 weeks gestation. What is the most appropriate next step in management?
A 24-year-old woman at 8 weeks of gestation presents with a history of pulmonary embolism 7 years ago during her first pregnancy. She was treated with intravenous heparin followed by several months of oral warfarin and has had no further evidence of thromboembolic disease for over 6 years. Which of the following statements about her current condition is true?
A gravida 3 female with a history of 2 previous second-trimester abortions presents at 22 weeks of gestation with cervical funneling. What is the most appropriate management?
Which of the following situations poses the greatest risk of Rh incompatibility?
What is the most reliable method for diagnosing fetal wellbeing?
Practice by Chapter
Fetal Assessment Techniques
Practice Questions
Hypertensive Disorders in Pregnancy
Practice Questions
Intrauterine Growth Restriction
Practice Questions
Multiple Gestation
Practice Questions
Rh Isoimmunization and Other Blood Group Incompatibilities
Practice Questions
Intrauterine Fetal Therapy
Practice Questions
Prenatal Diagnosis and Genetic Counseling
Practice Questions
Placental Abnormalities
Practice Questions
Preterm Labor and Delivery
Practice Questions
Management of Medical Disorders in Pregnancy
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app