
Maternal-Fetal Medicine — MCQs

On this page
Uterine height more than corresponding gestational age, with complaints of vomiting and pervaginal bleeding, favors which diagnosis?
What is the utero-placental blood flow at term?
A 4-month pregnant lady on regular treatment with valproate asks for advice regarding continuing the drug during pregnancy. What is the best course of action?
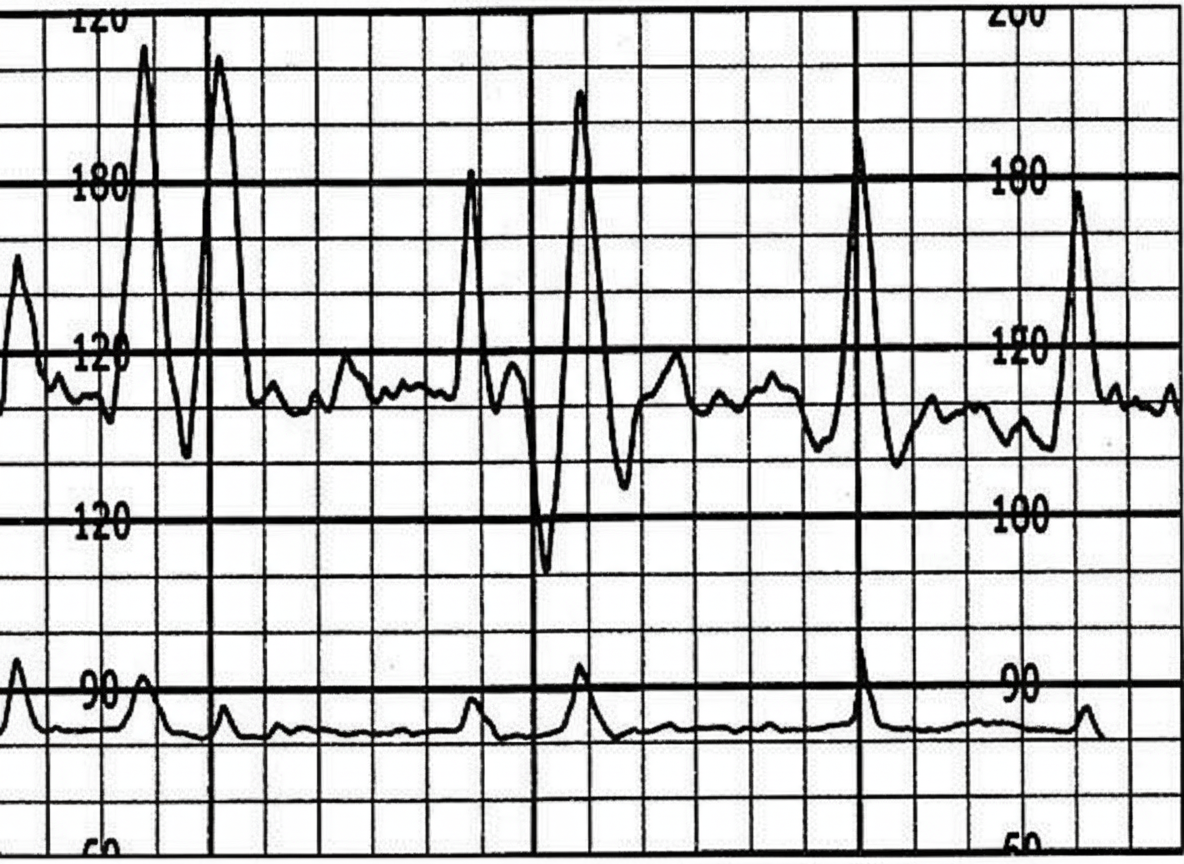
The following CTG indicates:
All of the following are true about cholestasis of pregnancy EXCEPT?
In pregnant diabetic patients, intrauterine fetal mortality increases after which week of gestation?
Which of the following treatments is not indicated in ectopic pregnancy?
Which congenital infection in a fetus carries minimal teratogenic risk?
A young female with 2 months of amenorrhea presents with sudden abdominal pain and an adnexal mass. Urine pregnancy test is positive. What is the most likely diagnosis?
A 29-year-old G3 P2 female at 32 weeks of gestation presents to the emergency department with a small amount of vaginal bleeding. She does not have any pain. Fetal heart rate tracings show fetal distress and late decelerations. What is the best course of action?
Practice by Chapter
Fetal Assessment Techniques
Practice Questions
Hypertensive Disorders in Pregnancy
Practice Questions
Intrauterine Growth Restriction
Practice Questions
Multiple Gestation
Practice Questions
Rh Isoimmunization and Other Blood Group Incompatibilities
Practice Questions
Intrauterine Fetal Therapy
Practice Questions
Prenatal Diagnosis and Genetic Counseling
Practice Questions
Placental Abnormalities
Practice Questions
Preterm Labor and Delivery
Practice Questions
Management of Medical Disorders in Pregnancy
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app