
Maternal-Fetal Medicine — MCQs

On this page
A 35-year-old G2P1L1 presents at 35 weeks of gestation with leakage per vagina. Examination of the pooled fluid shows it turns red litmus paper blue and exhibits ferning. The patient's temperature is 102 G2P1L1
All of the following is true about abruptio placentae except?
Which parameter on umbilical artery Doppler indicates imminent fetal demise?
A hypertensive primigravida with completely subsided pre-eclamptic features, up to what gestational age should the pregnancy be continued?
Betamethasone in pregnancy is given to prevent which of the following complications?
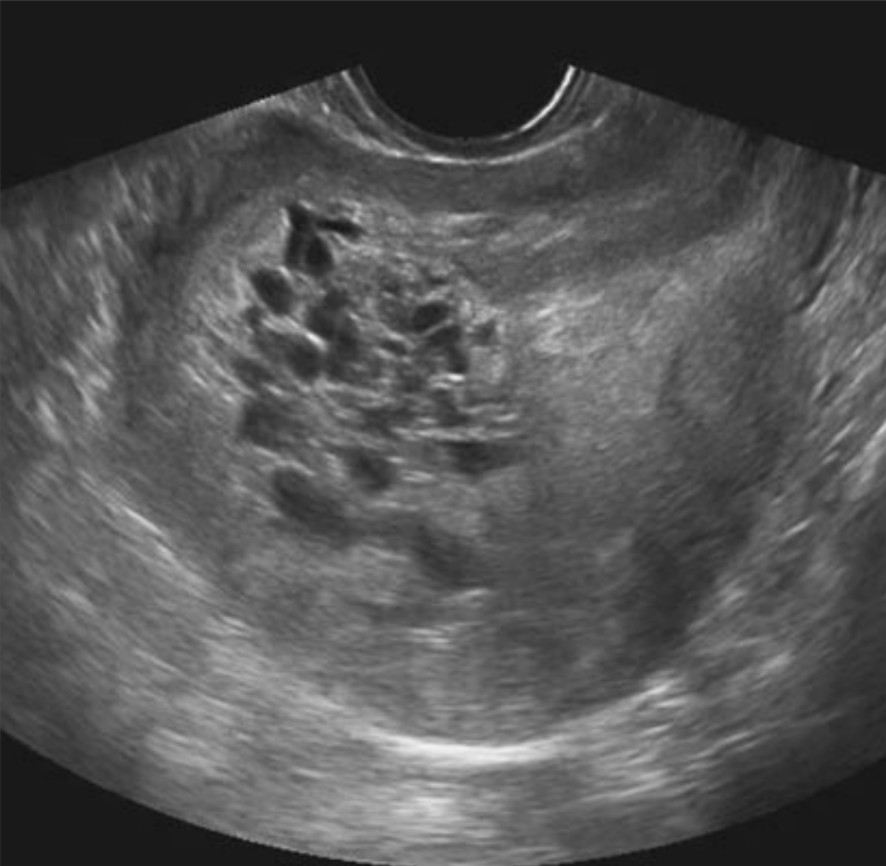
A 30-year-old primigravida complains of vaginal bleeding, pain in the abdomen, and vomiting. The uterus is enlarged, soft, and non-tender. Based on the ultrasound findings, what is the most likely diagnosis?
An 8th-month primigravida presented with severe pruritus and mild icterus. Her serum bilirubin was 3 mg/dL, with elevated AST, ALT, and alkaline phosphatase. Her renal function tests and coagulation profile were within normal limits. What is the most likely diagnosis?
Maximum cardiac output during pregnancy is typically observed at which gestational age?
All of the following statements about prenatal steroids are true except?
A woman presents with amenorrhea of 6 weeks duration and a lump in the right iliac fossa. What is the investigation of choice?
Practice by Chapter
Fetal Assessment Techniques
Practice Questions
Hypertensive Disorders in Pregnancy
Practice Questions
Intrauterine Growth Restriction
Practice Questions
Multiple Gestation
Practice Questions
Rh Isoimmunization and Other Blood Group Incompatibilities
Practice Questions
Intrauterine Fetal Therapy
Practice Questions
Prenatal Diagnosis and Genetic Counseling
Practice Questions
Placental Abnormalities
Practice Questions
Preterm Labor and Delivery
Practice Questions
Management of Medical Disorders in Pregnancy
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app