
Maternal-Fetal Medicine — MCQs

On this page
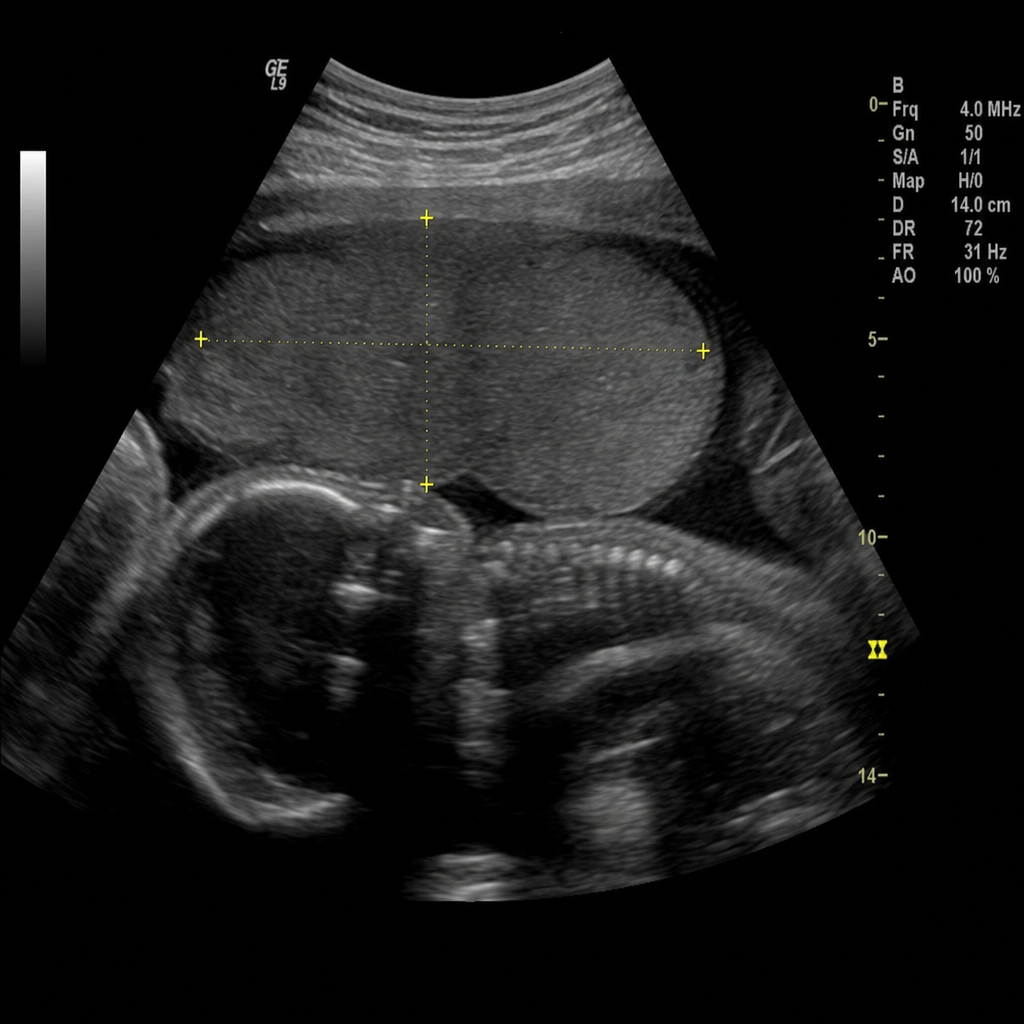
A 35-year-old multiparous lady at 30 weeks gestation presents with sudden onset painless vaginal bleeding. Ultrasound shows the following:
Which of the statements is FALSE regarding acute fatty liver of pregnancy?
Which of the following findings can be seen during clinical examination of a pregnant female with heart disease compared to a normal pregnancy?
Which of the following is not a criterion for antenatal diagnosis of Twin-Twin transfusion syndrome?
A 38-year-old woman is in her first pregnancy, which has been uneventful until the 34th week, when she develops swelling of feet and hands. An obstetric check-up reveals that she also has hypertension and proteinuria. Laboratory analysis shows elevated aspartate aminotransferase (AST) and alanine aminotransferase (ALT) and slightly decreased platelets. What is the initial event in the pathogenesis of her condition?
All of the following are true of placenta previa EXCEPT:
Which drug is given to prevent vertical transmission of HIV from mother to child?
Ventricular function improves with pregnancy in which of the following conditions?
Hypertension, proteinuria, and pitting edema are noted in the second month of the first pregnancy in a 25-year-old woman. The pathogenesis of her presenting complaints is most closely associated with which of the following?
Which of the following describes a dangerous placenta?
Practice by Chapter
Fetal Assessment Techniques
Practice Questions
Hypertensive Disorders in Pregnancy
Practice Questions
Intrauterine Growth Restriction
Practice Questions
Multiple Gestation
Practice Questions
Rh Isoimmunization and Other Blood Group Incompatibilities
Practice Questions
Intrauterine Fetal Therapy
Practice Questions
Prenatal Diagnosis and Genetic Counseling
Practice Questions
Placental Abnormalities
Practice Questions
Preterm Labor and Delivery
Practice Questions
Management of Medical Disorders in Pregnancy
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app