
Maternal-Fetal Medicine — MCQs

On this page
Large placenta is seen in all of the following conditions except?
Doppler ultrasonography in Intrauterine Growth Restriction (IUGR) and Preeclampsia shows a notch in which artery?
At what gestational age should an uncomplicated triplet pregnancy be delivered?
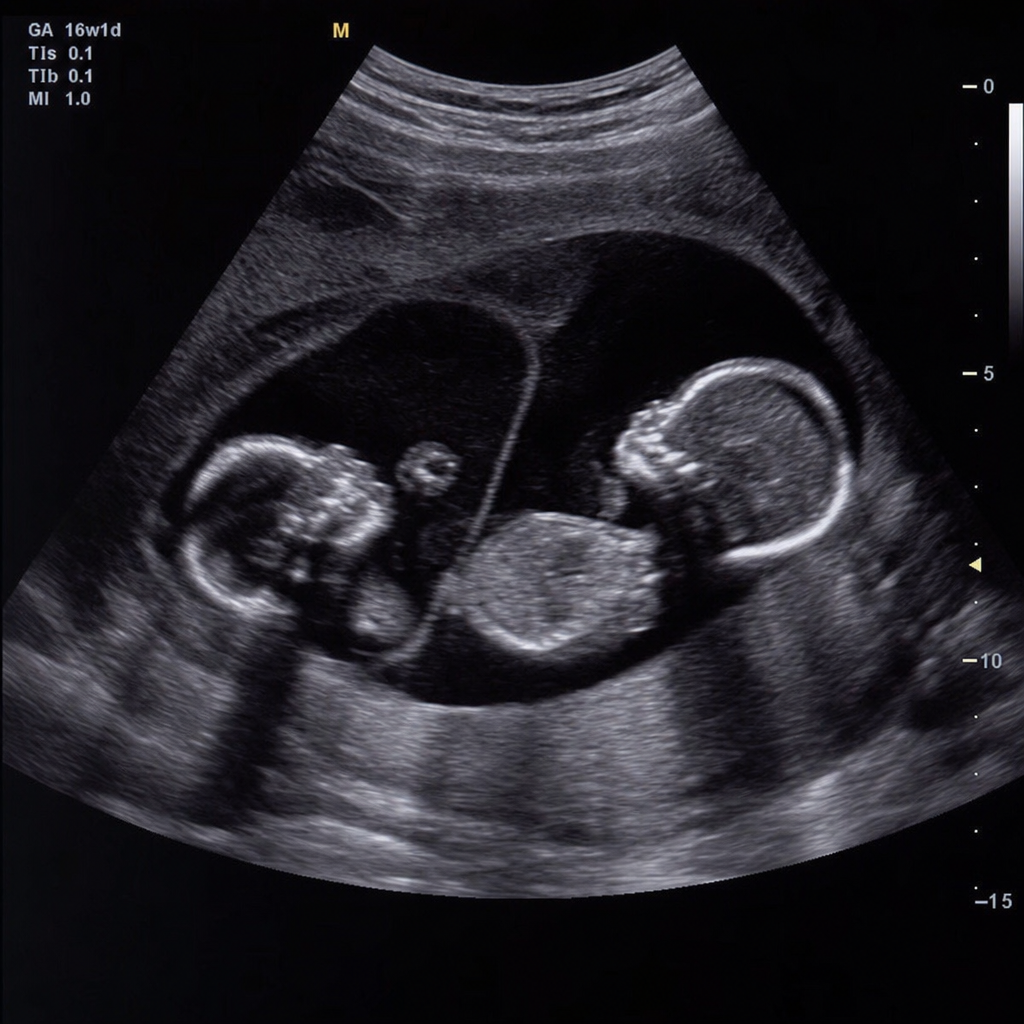
A 26-year-old primigravida with a twin gestation at 30 weeks presents for a USG. The sonogram indicates that the fetuses are both male and the placenta appears to be diamniotic and monochorionic. Twin B is noted to have oligohydramnios and to be much smaller than twin A. In this clinical scenario, all of the following are concerns for twin A except?
Is a dividing membrane present between the twins in this ultrasound image?
The risk of thromboembolism increases in pregnancy because:
A pregnant woman, G2P1, at 35 weeks gestation complains of decreased fetal movement. What is the next step in management?
All the following are true regarding HIV transmission from mother to infant, EXCEPT:
A primigravida presents with vaginal bleeding at term, but her vital signs are normal. What is the most appropriate management?
Which of the following strategies for administering magnesium sulfate for eclampsia prophylaxis should be used in the setting of an elevated serum creatinine?
Practice by Chapter
Fetal Assessment Techniques
Practice Questions
Hypertensive Disorders in Pregnancy
Practice Questions
Intrauterine Growth Restriction
Practice Questions
Multiple Gestation
Practice Questions
Rh Isoimmunization and Other Blood Group Incompatibilities
Practice Questions
Intrauterine Fetal Therapy
Practice Questions
Prenatal Diagnosis and Genetic Counseling
Practice Questions
Placental Abnormalities
Practice Questions
Preterm Labor and Delivery
Practice Questions
Management of Medical Disorders in Pregnancy
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app