
Maternal-Fetal Medicine — MCQs

On this page
What is the approximate percentage decrease in the chance of transmission of HIV to a fetus during pregnancy with the use of antiretroviral prophylaxis?
In which period of pregnancy is cordiocentesis typically performed?
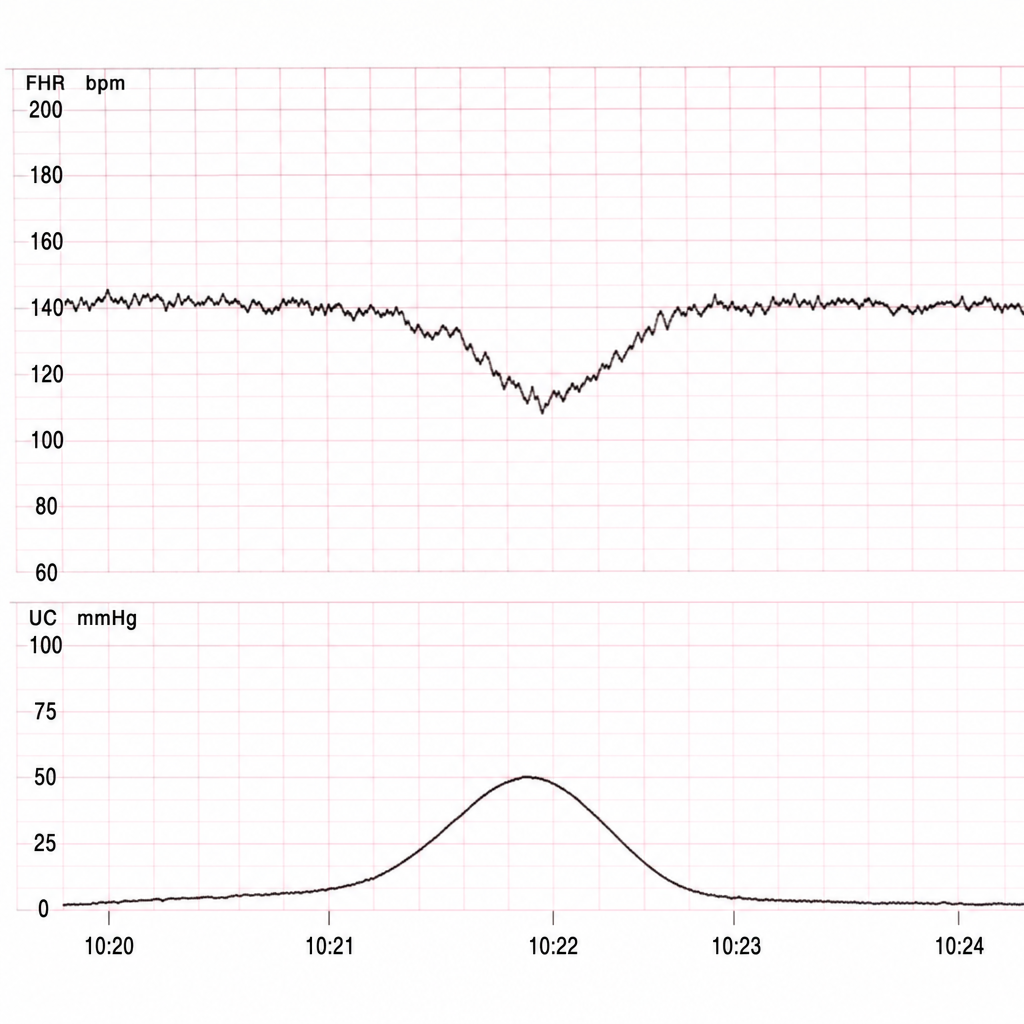
What does the CTG graph shown in the image indicate regarding fetal heart rate patterns?
Which of the following is seen in pregnancy with heart disease, which is not seen in normal pregnancy?
A pregnant woman presents at 22 weeks gestation for a routine prenatal visit. Physical examination demonstrates ankle edema and new onset hypertension. Urinalysis reveals marked proteinuria. Development of which of the following would justify a diagnosis of eclampsia?
What is the most common tumor of the ovary found in pregnancy?
Which of the following is a risk factor for pre-eclampsia?
A 25-year-old woman is G5, P0, Ab4. All of her previous pregnancies ended in spontaneous abortion in the first or second trimester. She is now in the 16th week of her fifth pregnancy and has had no prenatal problems. Laboratory findings include maternal blood type of A positive, negative serologic test for syphilis, and immunity to rubella. Which of the following laboratory studies would be most useful for determining a potential cause of recurrent fetal loss in this patient?
A 32-year-old G5P1 presents for her first prenatal visit. Classically, cervical incompetence is characterized by delivery in the second trimester preceded by which of the following?
What is the earliest sign of uteroplacental insufficiency detected by Doppler ultrasound?
Practice by Chapter
Fetal Assessment Techniques
Practice Questions
Hypertensive Disorders in Pregnancy
Practice Questions
Intrauterine Growth Restriction
Practice Questions
Multiple Gestation
Practice Questions
Rh Isoimmunization and Other Blood Group Incompatibilities
Practice Questions
Intrauterine Fetal Therapy
Practice Questions
Prenatal Diagnosis and Genetic Counseling
Practice Questions
Placental Abnormalities
Practice Questions
Preterm Labor and Delivery
Practice Questions
Management of Medical Disorders in Pregnancy
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app