
Maternal-Fetal Medicine — MCQs

On this page
All are complications of fibroid in pregnancy except:
Stillbirth is defined as the birth of a dead newborn child after how many completed weeks of gestation?
The theorized function of the Hyl anastomosis is equalization of which of the following pressure gradients?
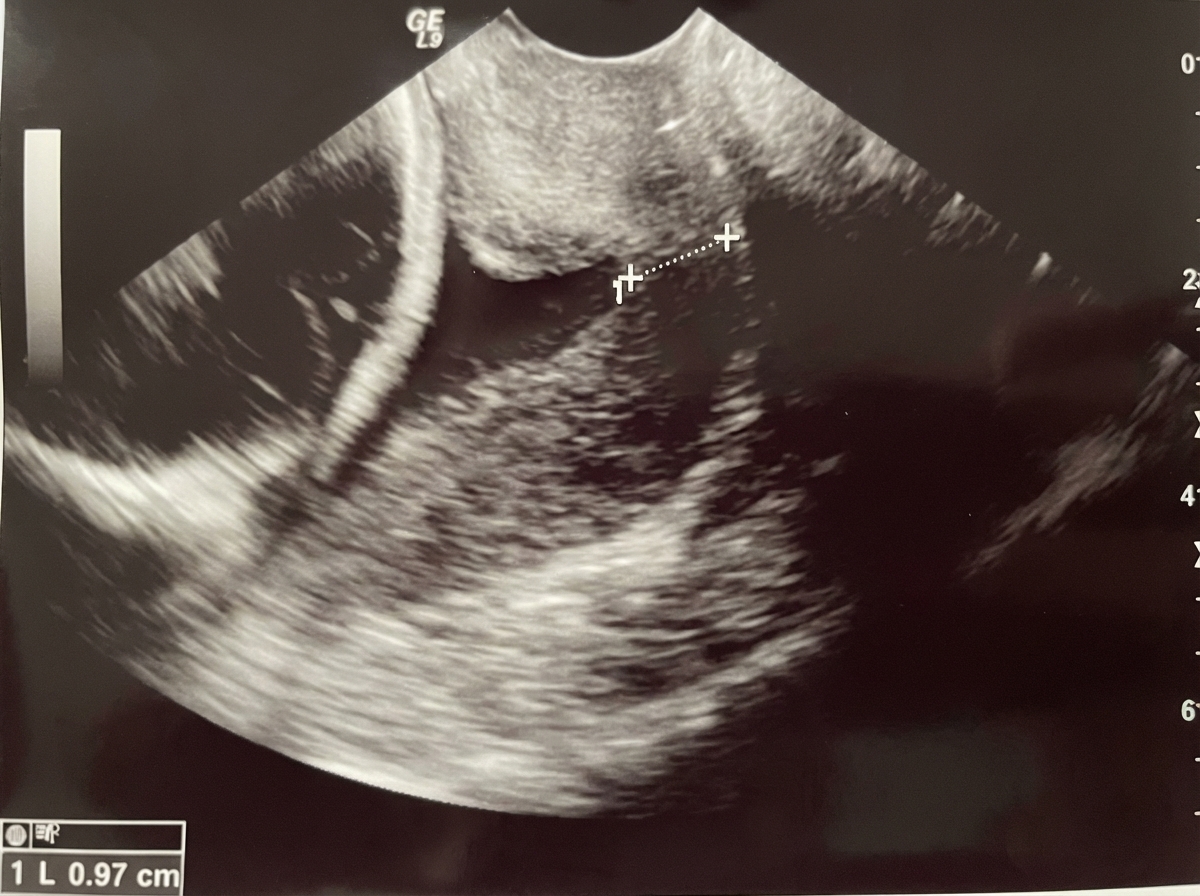
A gravida 3 female with a history of two prior second-trimester abortions associated with painless cervical dilatation presents with Level II ultrasound findings. What is the most appropriate management?
A G2P1L1 woman with a previous lower segment cesarean section (LSCS) presents at 37 weeks gestation with a blood pressure of 150/100 mm Hg. The cardiotocography (CTG) is reactive, and her per vaginum (P/V) findings are: os closed, cervix partially effaced, soft, midline, vertex at -2 station, and the pelvis is adequate. Urine protein by dipstick is 1+. What is the management?
Which of the following is a side effect of magnesium sulfate?
Which of the following is NOT an unequivocal evidence of heart disease in pregnancy?
Which of the following tests is not used for the detection of specific aneuploidy?
A pregnant woman presents with a major degree placenta previa and a malformed fetus. What is the best management approach?
A 25-year-old pregnant woman diagnosed with Rheumatic Heart Disease and Mitral Stenosis at 16 years of age presents at 6 weeks of gestation with a mitral valve area of 1.4 sq cm. She is currently in NYHA class 2 and on antiarrhythmic drugs. What is the risk of maternal mortality?
Practice by Chapter
Fetal Assessment Techniques
Practice Questions
Hypertensive Disorders in Pregnancy
Practice Questions
Intrauterine Growth Restriction
Practice Questions
Multiple Gestation
Practice Questions
Rh Isoimmunization and Other Blood Group Incompatibilities
Practice Questions
Intrauterine Fetal Therapy
Practice Questions
Prenatal Diagnosis and Genetic Counseling
Practice Questions
Placental Abnormalities
Practice Questions
Preterm Labor and Delivery
Practice Questions
Management of Medical Disorders in Pregnancy
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app